Introduction
The Avian influenza was first discovered in Asia. In isolated cases among poultry handlers, the Virus was transmitted from the birds to humans. However, researchers and scientists have found out the H5N1 virus has low virulence among humans and therefore downplayed fears that the virus in its current form would spark an epidemic feared. The World Health Organisation (2005) however noted a need that there was a need to keep the H5N1 virus on the watch because as other influenzas, the H5N1 virus could easily mutate to a form that would easily be communicable amongst humans. As a result, countries such as the United States and Britain issued travel alerts to their citizens to avoid travel to such countries unless it was completely essential to do so. Though players in the health industry do not issue travel advisories like governments do, they advise visitors to Asian countries to avoid contact with poultry or area where there are huge bird population (World Health Organisation, 2005). The medics also urge travellers to Asian countries to avoid eating poultry products, especially if they are not sure that such products have been adequately cooked.
Though statistics indicate that the human body is able to deal with the influenza virus and hence restore normal health, pandemics like those that hit the world in 1918 leading to million of casualties always raise concerns. Every time there is a new flu strain that appears in a particular region, people are cautious because they do not know whether the strain will be deadly or not. When the Avian flu first hit the headlines in 1997, it was reported that the virus was not easily transmitted from bird to humans, and even in cases where humans were infected, there were still doubts about the ease of transmission of the virus from one human to another (Cooper et al., 2006; Zitzow et al., 2002).
When respective governments issued travel advisories in the height of the Avian flu fears (Govorkova et al., 2005; WHO, 2005), and medics on the other hands issued precautionary measures that prevent infections, there seems to have been an admission that indeed people had a reason to be wary about the flu. As such, this affected travel to the Asian countries, especially among the older people. Apisarnthanarak et al. (2004) identifies the risk factors associated with H5N1 as old age, pneumonia, lymphopenia and leukopenia.
This study seeks to find out to what degree the influenza impacted elderly international tourism to Asian countries.
Hypothesis 1: H5N1 did not affect the elderly tourism demand to Asia because the confirmed cases on humans were too few to cause panic
Hypothesis 2: Elderly tourism demand to Asia continued unabated because the elderly population in Asia were the biggest participants in the same and therefore knew the reality on the ground
Literature Review
The first reported case of the avian flu in poultry was discovered in 1997 in Hong Kong. In the same year, 18 people were diagnosed with the virus, and 6 of them died (Wan et al., 2008). Six years later in 2003, the first two human cases (a father and son) was discovered in Hong Kong. The 33 year old infected man succumbed to the flu, but his son who was seven years at the time recovered.
Luckily, Osterholm (2005) notes that the spread of the H5N1 virus spread fast among poultry population in Asia than it did in humans. By 2005, Indonesia, Cambodia, Thailand and Vietnam collectively registered 112 cases of the flu among humans. Of these cases, 57 infected people succumbed to the virus. Unlike the first case where the older man died while his son recovered, the 57 deaths mainly occurred among children and the youth. Apart from one of the human infections; all other occurred to people who had handled poultry. As such, the research by Osterholm (2005) concludes that human-to-human infection of the avian flu is rare. This is with the exception of one suspected human-to–human infection that occurred in Thailand. Maines et al., (2005) states that an 11 year old child who had been admitted in hospital with the virus infected her mother who was taking care of her in the hospital. The mother had no prior contact with chickens.
According to the World Health Organisation (2005), the H5N1 virus was of particular concern to people influenza for two reasons: first, the pathogen in the virus was able to pass to humans from poultry; and secondly, there was a high likelihood that the virus would be transmitted from amongst humans. The second reason made WHO and health experts worldwide believe that the virus had a potential to ignite a global pandemic. To make matters worse, the virus had shown a 50 percent risk of death in humans.
Lam (1998) argues that Asia is seen as the epicentre of new influenza strains, and the emergence of the avian flu in Hong Kong supports this contention. He also notes that the Asian governments have a history of failing to handle emergence of health issues competently especially because they lack the necessary surveillance programs. Lam (1998) further notes that the sensitive nature of the tourism industry means that reports regarding such flu would cause panic among travellers especially when they perceive their age or health as a risk factor that would place them at a higher risk of contracting the virus.
The World Bank (2005) noted that there were great uncertainties regarding the virulence, the timing and the general scope of a possible human flu pandemic in Asia. “Best case scenarios modelled on the mild pandemic of 1968, project global excess deaths on the range of 2 million to 7.4 million…. should a more virulent virus attack, the numbers could go as high as those registered in the 1918 pandemic” (WHO, 2005). The report further indicates that epidemiological, clinical and laboratory evidence gotten from H5N1 virus suggest that if the virus assumed a human to human transmission, the resulting infections would easily mimic what happened in the 1918 pandemic. Basing the number of visitors who tour Asia annually, W.H.O. estimates that at least the United States would have at least 1.7 million deaths if a virus strain that is easily transmitted amongst humans was to occur. The other parts of the world would register 180-360 million deaths, with the highest concentration of deaths being in Asia and other countries whose population contribute significantly to Asia’s tourism sector.
Interestingly, World Health Organisation (2005) notes that the greatest economic impact on the Asian economies would not happen from the deaths that would occur during the pandemic, but would occur from the “uncoordinated efforts of private individuals as they try to avoid infections” (p. 2). This deduction by WHO is based on similar observations in the past where news about virus infections hit the media headlines. As people try to minimize face to face interactions, demands in the services sector especially in tourism and related sectors significantly goes down. In an attempt to shield the public from infections, governments react similarly by issuing travel advisories in an attempt to shield their own economies from the costs that would occur if such infections were to spread in to their domestic environments (Osterholm, 2005).
Osterholm (2005) note that the tourism declining levels witnessed at the height of the 2005 Avian flu fears were as a result of panic, which was magnified by lack of proper and accurate public information. The misinformation led to private individuals in the oversee tourism industry over-estimating the perceived probabilities of the virus infection or death. Consequently, potential tourists to Asian countries would then take preventative actions, which in most cases was to avoid or postpone travel until such a time when the H5N1 virus was not a threat anymore.
According to the World health organisation (2005), governments issued travel advisories to Asian countries at the height of the 2005 avian flu fears based on the need to “curb the flu at source” (p. 3).
Older tourists have a reason to keep off areas that have a high risk of flu infections because as Meltzer et al. (2005) notes, age is in itself a risk factor to flu. Persons aged 65 years and above are more prone to illnesses and deaths than the younger population. Chen & Wu (2008) carried a study that concluded that elderly people have the time and resources to spend on travel. Their study also found that baby boomers and other people in the population who have hit retirement age make a significant population the world over and therefore would be expected to form a significant percentage of tourists in different travel destinations. Although the elderly tourists may not take part in some of the physically challenging tourism activities offered in different countries in Asia, Chen and Wu (2008) observes that there is a high likelihood that medical tourism would act as a major attraction to them.
Uysal (1998) notes that the image of a travel destination is one of the social-psychological factors that affect elderly travel trends. This means that a travel destination that has a tainted image would receive fewer visitors from the international market. Relaxing and socializing are also cited as factors that motivate international tourism (Chen & Wu, 2008). This however would seem like an unlikely motivation in the wake of travel advisory advising travellers to be cautious when visiting specific places.
Rossi & Walker (2005) states that tourism encourages discretionary spending on global travel and leisure pursuits and hence contributes significantly to the Asian economies. However, it is notable that the Avian flu (either because of the few reported casualties or the fact that government simply issued travel advisories rather than travel bans) did not affect tourism even among the elderly as would have been expected. In the SARS cases, a country like Thailand had their tourism industry negatively affected. This however was not witnessed in the case of the avian flu. Ideally, Rossi & Walker (2005) states that the hype created by the media, respective governments and other stakeholders in the health industry would result in lowered visits by foreign tourists into the Asian countries. Notably, even tourists who would visit the Asian countries would stay for shorter periods thus meaning that there spending would reduce significantly when compared to other times.
As stated out in the WHO (2005) study, age is in itself seen as a risk factor in contracting of flu. Rossie & Walker (2003) observes that older tourists have much more money to spend than the backpackers who usually travel on budget. Retirees (60 years and older) usually have more time to spend in their holiday destinations. They are also more likely to spend time on shopping trips and restaurants rather than engaging in some of the other physically taxing tourism activities. With travel alerts however, this would be more likely to change.
Description of Terms
H5N1: Influenza A, subtype H5N1. This influenza subtype is also known as avian flu or simply bird flu. The causative virus has been found to cause illness in human beings but there have been no cases of human-to-human transmission albeit fears that such an occurrence would cause a global flu pandemic.
Severe Acute Respiratory Syndrome (SARS): A respiratory disease caused by SARS coronavirus. Between November 2002 and July 2003, 8093 people were infected with the SARS virus, which lead to 774 deaths across 37 countries where the disease had spread to. According to WHO (2005), elderly people had a more than 50 percent chance to die from the infection while younger people registered lower risk rates.
Virulence: The extent to which a pathogen can cause disease in humans.
Methodology
To collect data, this study will use travel statistics published in different internet bases to gauge the difference in tourism patterns in three years: 2004, 2005, and 2006. These three years were chosen specifically because 2005 was the height of the avian flu cases. One would therefore expect that there would be noticeable changes in tourism arrivals in specific Asian countries. The tourism arrivals will then be examined along demographics in order to establish if indeed the elderly refrained from visiting specific Asian countries.
The study defines the elderly tourist as any tourist aged 65 years or older.
Research Model
This study seeks to gather quantitative data from different websites that have recorded statistics that reflect the inbound tourism trends in specific Asian countries. The method used in analysing data will be deductive in nature and the reliability of the data collected from different websites will be compared in order to establish the authenticity of the same. A literature review has been conducted in order to gain insight on the existing variables, theories and deductions made by other researchers.
Findings
China
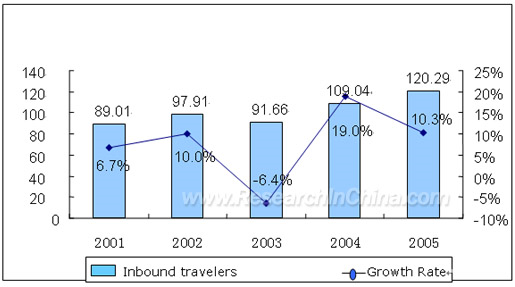
China was among the countries that were receiving media attention related to avian flu. The first case was discovered in Hong Kong as indicated elsewhere in this study and poultry farms continued to register high deaths due to the effect of the H5N1 on chickens. Notably however, China’s tourism sector was at its lowest in 2003 courtesy of SRAS fears. In 2004 however, the inbound tourism numbers rose tremendously. In 2005, the tourism sector performed even better recording a 10.3 percent growth from 2004. This translated 120.29 million inbound travellers. 20.6 million Travellers came from the oversee countries while the remainder numbers was made of tourists from Taiwan, Macau and Hong Kong (Research in China, 2009). Tourists from Europe accounted for 10.2 percent of tourism arrivals in 2005, while America, Africa and Oceania accounted for 10.2 percent, 11.3 percent and 12.1 percent respectively. According to Research in China (2006), arrivals from Canada increased by 16.9 percent from the previous years, while Australia’s visitors to the country increased by 11.4 percent. The arrivals from US and Germany were 10 percent higher each.
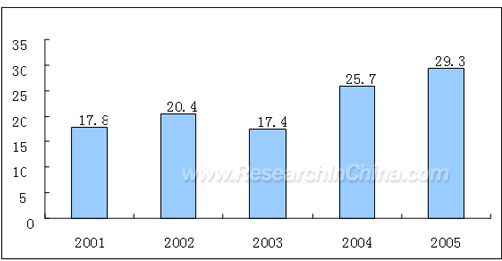
Research in china (2010) further indicates that foreign exchange from international tourism was at its highest in 2005 with 29.3 million US dollar earned in that period. In 2004, the country had earned 25.7 million US dollars from tourism and 17.4 million US dollars in 2003.
A notable characteristic of foreign tourists to china is that the elderly (65 years and older) are just a fraction of the visitors. Out of the 26.1 million visitors to China in 2007 for example, only 1.52 million were 65 years or older. Most visitors came from the 45-64 years age group accounting for 9.5 million visitors (China Tourism Statistics, 2010).
Singapore
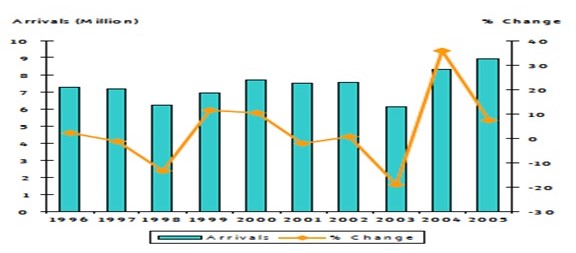
In a similar trend to the one observed in China, Singapore’s inbound tourism was at an all time low in 2003. This was mainly because of the SARS related fears that meant that travel within Asia or to Asia from other countries adopted a cautious approach. In 2003, Singapore had 6.1 million international visitors, which was followed by a steep rise of 35.9 percent in 2004 translating to 8.3 million visitors. In 2005, the increase continued although it slowed down to 7.4 percent growth from the previous year translating to 8.9 million visitors in 2005. In 2006, Singapore had 9.8 million inbound tourists, which was a 9.0 percent growth from 2005. Amazingly, Singapore is perceived as a viable medical tourism destination by the elderly within the Asian continent and elsewhere in the world where a balance between cost and professionalism is offered (Singapore Tourism Board, 2005).
Just like china, the bulk of inbound tourists to Singapore were from the Asian countries. Collectively, South Asia, North Asia, West Asia and Southeast Asia accounted for 74 percent of all tourists who visited Singapore in 2005. Europe accounted for 12 percent of all tourists to Singapore in 2005, while Oceania contributed 8 percent of the inbound tourists. The American tourists accounted for 5 percent of the total arrivals, while Africa accounted for 1 percent of the arrivals (Singapore Tourism Board, 2006)
Singapore statistics indicate that visitors aged 65 years and above contributed a mere 6.4 percent of the collective tourism arrivals. The average age in arrival was 34.7 years with the highest number of visitors coming from the 35-44 years age group (Singapore Tourism board, 2006).
Analysis
Comparing the tourism trends in Singapore and china, they draw a similarity in:
- Most inbound tourists in both countries were mainly from Asian countries
- Both markets had suffered significantly from the SARS attacks in 2003
- Both countries marked significant recovery in 2004
- Tourism in both countries continued in an upward growth path in 2005
Analysis in to the elderly tourism trend suggests that there was no much difference between percentages recorded in 2004 and 2005. The overall tourism increase corresponded with the same in the elderly tourists. Notably, there was no decline in tourism arrivals in both countries.
There are several possible explanations for the observed resilience of elderly tourism in Asia in 2005:
- The elderly tourists, just like other younger tourists did not take the travel advisories offered by their respective government regarding travel to Asia. Ostensibly, the few number of human casualties was most likely perceived by the general population that the H5N1 virus was yet to mutate to a form that could easily be transmitted between humans.
- The health sector continued surveillance and the release of information to the media regarding the isolated cases that only occurred in humans who had been in direct contact with infected chicken could also have downplayed the seriousness of the virus and rightfully so.
- The fact that the virus had not been transmitted from human-to-human since 1998 when the first case was discovered may have been perceived as an indication that it was nearly impossible for the virus to all of a sudden assume a virulence that would easily be transmitted amongst human beings.
- The elderly tourism market in Asia draws visitors from Asian countries in the continent. This probably describes the resilience portrayed by the elderly because they knew they were just borders away from each other. As such, tourism or not could not prevent the spread of the disease if it actually became a pandemic. As such, one would assume the elderly adopted a “why not enjoy it now” attitude.
Challenges in Data Collection
This study was handicapped by the lack of published data on age-related tourism trends. For example, although there was data detailing the number of visitors aged 65 years and above visiting both Singapore and China in 2005, there is no data showing where those visitors came from. The study is therefore working on assumption that just as the majority of inbound tourists in both countries was from Asian countries, so did the elderly tourist. If this is the case then, the hypothesis 1 in this study would have been proven because there seems to have been little apprehension among Asian nationals to visit other countries within the continent even in the height of SARS (WHO, 2005).
Conclusion
Tourism is a very sensitive industry. Negative publicity of a tourist destination often always results in decreased tourisms. More so, the slightest risk, especially in regard to human safety (disease, terrorism etc) is enough to spur a drastic change of fortune for tourism destinations. This study therefore finds it quite out of the ordinary that the elderly tourism market to Asia did not suffer any drastic effects at the height of the 2005 avian flu fears. Through observations made in the course of the study, this study concludes that tourists make their travel decisions based on careful consideration of facts. To this end, this study observes that the lack of many deaths in Asia did not provide the tourist with convincing evidence that Asia was worth keeping off in 2005. This conclusion is made from an informed position considering the effects of confirmed infections such as those observed in 2003 at the height of SARS.
References
Apisarnthanarak A, Kitphati R, Thongphubeth K, Patoomanunt P, Anthanont P, & Auwanit W. et al. (2004). Atypical avian influenza (H5N1). Emerging Infectious Diseases Journal 10(7), 1-12.
Chen, C. and Wu, C. (2008). How Motivations, Constraints, and demographic factors predict seniors’ overseas travel propensity. Asia Pacific Management Review 14(3), 301-312.
China Tourism Statistics (2010). China Tourist Office. Web.
Govorkova, E.A., Rehg, J., Krauss, S., Yen, H, Guan, Y et al. (2005). Lethality to ferrets of H5N1 influenza viruses isolated from Humans and Poultry in 2004. Journal of Virology 79(4), 2191-2198.
Maines, T.R. Et al. (2005). Avian Influenza (H5N1) Viruses isolated from humans in Asia in 2004 exhibit increased virulence in mammals. Journal of virology 79(18), 1178-11800.
Meltzer, M. I., Cox, N. J. & Fukuda, K. (2005). The economic impact of the pandemic influenza in the United States: priorities for intervention. Emerging infectious diseases Journal 5(5), 1-9.
Osterholm, M. T. (2005). Preparing for the next pandemic. New England Journal of Medicine 35 (25), 1834-1839.
Research in China (2006). China Industry report. Web.
Rossi, V. & Walker, J. (2005). Assessing the Economic Impact and the costs of Flu pandemics originating in Asia. Oxford Economic Forecasting Ltd. Web.
Singapore Tourism Board (2006). Annual report on Tourism Statistics2005. Web.
The World Bank (2005). Spread of Avian flu could affect next year’s economic outlook. Web.
Uysal, M. (1998). The determinants of tourism demand: A theoretical perspective. In Ioannids,D., Debbage, K. (Eds.) The Economic Geography of the Tourist Industry: A Supply Side Analysis. Routledge: London.
Wan, X, Nguyen, T, Davis, T, Smith, C et al. (2008). Viruses in Vietnam between 2001 and 2007. Pubmed central journal 3(10). Web.
World Health Organization. (2005). Avian Influenza: Assessing the Pandemic Threat. WHO/CDS/2005.29.
Zitzow, L.A, Rowe, T., Morken, T., Shieh, W et al., (2002). Pathogenesis of Avian Influenza A (H5N1) viruses in Ferrets. Journal of Virology 78(9),4420-4429.