- Introduction
- Description of the ASI, Its Purpose, and Functions
- The Role of the Interviewer
- Severity Ratings in the ASI: The Meaning and Process
- The Adaptation of the ASI: Areas to Retain or Change
- Appending Additional Information
- Effectiveness of the ASI in a Community Clinic Setting
- Conclusion
- Reference List
Introduction
The Addiction Severity Index (ASI) as a tool for measuring the severity of alcohol and drug addiction in adult patients can be used by community health workers for the assessment of representatives of ethnically and culturally diverse groups. In order to achieve the assessment goals, it is important to provide recommendations for using the ASI while measuring the addiction status of Native Americans in the context of a community clinic setting. The purpose of this training workbook is to present the guidelines on using the ASI and its adapted form when working with the Native American population.
Description of the ASI, Its Purpose, and Functions
The ASI is an interview-based instrument for assessing adults’ substance use disorders that were developed in 1980. The purpose of the ASI as a standardized and valid tool is to measure the severity of a patient’s addiction referring to such areas as the medical status of a person, his or her employment and support status, drug and alcohol use, legal status, family, social status, and psychiatric status (Carise, n.d.). The information on a patient’s state should be collected during a one-hour semi-structured interview reflecting on a person’s recent and life problems. Community health workers should remember that the assessment usually functions as the first measuring tool that is used to provide an overview of a patient’s problems related to alcohol and substance use. There is no concentration on a single area in the assessment, and a counselor receives broad information on a person’s urgent problems and chronic issues. When applying the ASI to working with diverse populations, including Native Americans, it is necessary to modify the tool while adding more questions related to social and spiritual aspects.
The Role of the Interviewer
The role of a counselor in conducting the ASI interview is very important because the assessment is significantly based on an interviewer’s subjective evaluation of the level of severity regarding alcohol and substance abuse (severity ratings) utilized for determining interventions. Therefore, an interviewer is expected to understand the meaning and intent of each question in the protocol, and he or she is responsible for guaranteeing the integrity of the collected data (“Addiction Severity Index,” 2014). An interviewer also makes sure that a patient understands the question to provide an adequate answer. It is necessary to review all questions before starting an interview, consult the manual for the ASI, make notes regarding the areas to pay attention to and collect information on interacting with a specific diverse group. While working with Native Americans, an interviewer should be aware of their cultural specifics, concern areas, and communication patterns to build positive and secure relationships with patients and avoid possible barriers to interaction. Thus, interviewing a Native American, a counselor is expected to be supportive, unbiased, and honest.
Severity Ratings in the ASI: The Meaning and Process
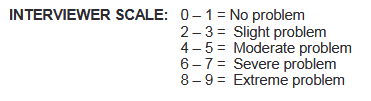
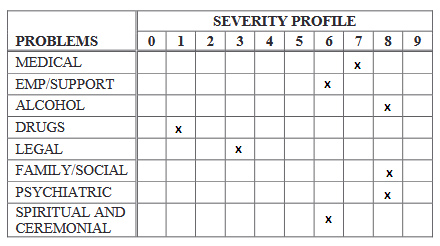
While assessing the severity of a patient’s problem with substance use, an interviewer refers to confidence, patient, and severity ratings. A counselor needs to pay much attention to severity ratings which are usually optional for the assessment, but they are still important for deciding on interventions. Severity ratings are subjective ratings made by an interviewer regarding a patient’s need for receiving some kind of treatment. Referring to the duration of the discussed symptoms and their intensity, an interviewer is expected to assign the score to different areas ranging from 0 to 9 (Hays, 2017). Counselors should remember that 0-1 indicates that no specific treatment is required, and 8-9 accentuate the extreme need for treatment (Figure 1). High severity ratings demonstrate a person’s need for treating his or her symptoms and problems. The same process is used while assigning scores for the problems of patients of Native American origin.
The Adaptation of the ASI: Areas to Retain or Change
The adaptation of the ASI for interviewing Native Americans is based on the following aspects: the key problem areas are retained with slight modifications regarding the formulation of questions and one more area on spiritual and ceremonial practices should be added to the protocol. The basic form of the ASI protocol remains without changes, and the key areas are retained. The number of the main seven areas or sections in the protocol should also remain unchanged (“Addiction Severity Index,” n.d.). It is also important to note that the deletion of basic questions in the ASI is not recommended because this protocol is designed to gather the minimum information regarding a client’s recent state and lifelong problems. In this case, inappropriate questions can be reformulated to address a specific diverse group (Carise, n.d.). Different adaptations of the ASI, including the ASI for Native Americans, contain modified questions within the mental status, employment/support, drug/alcohol use, and other areas. Sections are changed according to the needs of local health care facilities where the ASI is applied.
The adapted versions of the ASI can include culture- or community-specific questions in order to understand how unique backgrounds can influence the development of problems in a patient. Thus, appropriate questions are usually added to the basic list of points, and these modified variants are available in several languages. In the adaptation of the ASI for Native Americans, the medical status section can comprise questions on tribal medicine in order to understand whether a patient uses the medical assistance related to the Native American culture and traditional medicine (Carise et al., n.d.). The section on employment and support can have added questions on traditional education in reservations, and questions about the sources of money can be modified or united in one general question to avoid embarrassing a patient. The section on family and social relations can include the modified genogram for representing problems in a patient’s family members to record the provided information in the most appropriate manner (Carise, n.d.). This section can be expanded to include the questions on the specifics of a patient’s life in a reservation in terms of duration and the overall level of satisfaction.
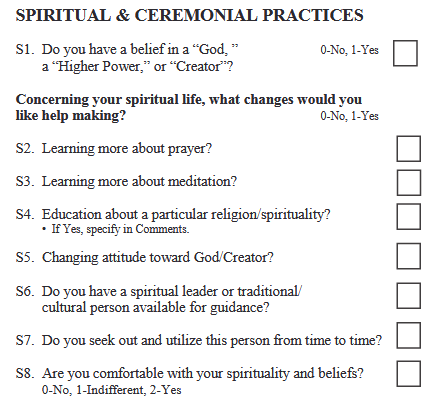
One more important modification for the ASI protocol used for interviewing Native Americans is the Spiritual and Ceremonial Practices section. This section and related questions are added to the ASI interview in order to provide an interviewer with information on how a patient’s spiritual practices can influence his or her alcohol consumption and drug abuse, increasing or not the severity of problems (Figure 2; Carise et al., n.d.). If this section is added to the ASI protocol, an interviewer is expected to treat a patient with respect when asking about his or her spiritual and ceremonial practices. Similar sections can be added to other ASI versions depending on the cultural backgrounds in which this assessment tool is planned to be used.
Appending Additional Information
Interviewers should pay attention to the fact that any questions that are added to modified versions of ASI protocols are assigned with additional numbers that were not initially used in the ASI form. Thus, the numerical order of questions in sections can be broken to identify new questions (Carise, n.d.). If it is required to add one more section, as it is in the case with the ASI version for Native Americans, this section follows the mental status, employment/support, drug/alcohol use, family/social relations, legal status, and psychiatric status sections. Any other information that can be added to the ASI protocol as appendices follow the key sections. This appended information can include a list of the major problems identified in a patient and a treatment plan with related objectives.
Effectiveness of the ASI in a Community Clinic Setting
Counselors should focus on the idea that, in a community clinic setting, they are expected to cooperate with a large group of community representatives who can influence each other because of tight family and social relations. Specific communities can have a significant positive or negative effect on patients, and this aspect should be taken into account while working with alcohol consumers or drug-addicted persons. The use of the ASI in a community clinic setting allows for focusing on particular features of the background in which a patient lives. With the focus on the experience of Native Americans living in reservations, communities can have a unique significant impact on the behavior and choice of individuals (Venner et al., 2016). Therefore, the ASI is effective to be used in this context because it allows for overviewing a patient’s social background, family relations, as well as his or her role in a community and the received social support.
Comparing the use of the ASI in this clinical setting to applying the tool in a private practice setting, it is important to note that a patient can avoid providing much detail regarding his or her social life, and the absence of information regarding the community does not allow for receiving a full picture. ASI protocols developed for diverse cultural or ethnic groups to be used in different communities can be more detailed than a basic form of the ASI protocol. As a result, the effectiveness of the measurement instrument adapted to a certain community clinic setting can be higher in comparison to the outcomes of using the ASI in a private practice setting.
Conclusion
This training workbook has presented detailed information on how to use the ASI tool for assessing patients who belong to diverse racial and cultural groups. This workbook has been focused on providing the guidelines for the ASI application in the context of a community clinic setting with a concentration on the needs of Native Americans. As a result, the details on how to adapt the ASI protocol to the needs of the Native American population are presented with reference to the general purpose of this measurement tool and controversies regarding the application of severity ratings. The areas that should be retained in the ASI form or changed according to the population’s characteristics have been described, and the notes on appending additional information have been made in this workbook that can be used by counselors working in Native American reservations.
Reference List
Addiction Severity Index. (n.d.). Web.
Addiction Severity Index: Treatment planning manual. (2014). Web.
Carise, D. (n.d.). Addiction Severity Index revised user’s guide – North Dakota State adaptation for use with Native Americans. Web.
Carise, D., Wicks, K., McLellan, A. T., & Olton, P. (n.d.). Addiction Severity Index 5th edition – North Dakota State adaptation for use with Native Americans. Web.
Greenfield, B. L., Hallgren, K. A., Venner, K. L., Hagler, K. J., Simmons, J. D., Sheche, J. N.,… Lupee, D. (2015). Cultural adaptation, psychometric properties, and outcomes of the Native American Spirituality Scale. Psychological Services, 12(2), 123-131.
Hays, D. G. (2017). Assessment in counseling: Procedures and practices (6th ed.). New York, NY: John Wiley & Sons.
Padyab, M., Armelius, B. Å., Armelius, K., Nyström, S., Blom, B., Grönlund, A. S., & Lundgren, L. (2018). Is clinical assessment of addiction severity of individuals with substance use disorder, using the Addiction Severity Index, a predictor of future inpatient mental health hospitalization? A nine-year registry study. Journal of Dual Diagnosis, 1, 1-16.
Smith, R. L. (2015). Treatment strategies for substance abuse and process addictions. New York, NY: John Wiley & Sons.
Venner, K. L., Greenfield, B. L., Hagler, K. J., Simmons, J., Lupee, D., Homer, E.,… Smith, J. E. (2016). Pilot outcome results of culturally adapted evidence-based substance use disorder treatment with a southwest tribe. Addictive Behaviors Reports, 3, 21-27.