Abstract
Recent national data point to the fact that substance abuse among adolescents did not change significantly over the past decades despite the volume of prevention and intervention programs. Frontier communities have specific socioeconomic and cultural characteristics which put frontiers adolescents at high risk for substance abuse.
This work aims at reviewing the issue of adolescent substance abuse focusing on frontiers communities and presenting a preliminary assessment of the efficacy of Dr. Gil Botvin’s Life Skills Training Program for the middle schools’ student population of Oregon. As many researchers confirmed the school is the primary site to target this problem. The researcher examined the effects of applying Botvin Life Skills Training in Lake County, Oregon middle schools over the period October 1998 to February 2000.
One hundred thirty three 6th grade adolescents and 99 7th grade adolescents were provided with self-report questionnaires before and after implementing life skills training. The Survey included 11 questions chosen from sections C and D of the survey prepared by Cornell University designed to measure self-reported substance abuse, student perception of drug abuse among peers and adults, drug refusal skill, and decision making skills.
Other measures included were media effect, anxiety reduction mechanisms among adolescents examined, and communication skills. Overall analysis of results showed that6th graders are more responsive to life skills training and the need to a multifactor prevention approach considering specific risk and protective factors in Lake County. The data also suggest the potential of interactive approach in preventing substance use in young adolescents.
Introduction and background
Youth drug use and abuse is becoming a growing social and a public health problem that attracted great public concern, which resulted in a national clamor for influential prevention and intervention programs. There are many substances blamed to be of use and abuse by adolescents. Substances are categorized into licit or lawful (bought legally as tobacco and alcohol) and illicit or illegal as heroin, cocaine, amphetamines, or cannabis. This has influenced public and individual perception to the whole problem. First, the public perception on a drug being a licit one is there are no sufficient motives to face its consumption. Second, being licit, it is available for adolescents’ wide use; yet, the harm is still cropping up.
There are three main patterns of how people look at an adolescent drug user. First, the user is a morally or religiously defective person (committing a sin or a social offense). The second pattern views the user as an ill person who needs medical or psychiatric help. The third pattern considers the user as a socially injured person who passed or is passing through hardships. However, all these interpretations focus on the individual. Proper understanding of adolescents’ substance use mandates dealing with all sides of the problem, which are the drug, the individual, and the environment (Fagg, 2006).
It is important not to avoid dealing with the problem of adolescents’ drug use, since it results in harmful effects on the individual’s behavior, personality with resultant serious social and health outcomes. Besides the substance’s health adverse effects, adolescents are in a stage of behavior and brain functioning development. Therefore, the results may affect the present individual’s life and in the future (Watkins and others, 2006). According to Burrow-Sanchez (2006), there are four areas to deal with this problem on an individual level. First, a counselor, peer, or a family member needs to setup a valid relationship with the adolescent.
Second, authorities have to evaluate the problem from all sides, about the substance, the individual, and the social environment. Third is, for social workers to realize the possibility of recurrence (relapse). Finally, a counselor needs to consider the various treatment approaches based on a comprehensive assessment if the adolescent passes to abuse or dependence. Figure (1) elicits the problem volume and shows Drug use rates by age in the US (based on National Household Survey on drug use, 2000, cited in the report of the Office of National Drug Control Policy (a), 2002).
Influential prevention and intervention programs should also prevent progression of the problem from abuse to addiction, and center on the problems associated with substance use and abuse whether behavioral, criminal, psychological, or health problems. Various programs ranging from simple one time intervention (in a single area locality) to nationwide network programs developed to address these objectives. These programs’ arrays of any range share the lack comprehensive and reliable evidence that they work effectively. In addition, the lack of information on epidemiology and etiology of substance abuse in rural and frontiers areas holds back informed decision making about intervention strategies in these areas (Robertson, 1997).
In an extended review, D’Onofrio (1997, in Robertson et al [editors] pp. 250-346) inferred the pattern of alcohol use among adolescents is similar across different areas considering population density. Further D’Onofrio (1997) studied the limited literature of adolescent substance use in rural areas and suggested that various risk factors like personality characteristics, peers and family influence, and age of initiation are similar to those in urban areas.
Despite the likenesses in epidemiology and etiology of adolescent substance use across different areas there is no or little evidence that universally designed prevention programs can be applied to different areas’ setting with success. Thus, there are two conflicting viewpoints; one argues that such programs can be applied with success if proper procedural methods are followed. Another outlook suggests community tailored prevention programs should be adopted according to the risk and protective factors of that community (D’Onofrio, 1997).
In 2003, Johnston and colleagues (NIH publication number 03-5374) analyzed data from the 2002 Monitoring the Future Study about adolescents substance use. They inferred that overall pattern of drug use of eighth to 12th graders is nearly the same across areas, and the trend remains consistent in elder adolescents. The data also confirmed that adolescents remain a high risk group for drug use. They recognized a major criticism to universal prevention programs is the lack of focus on community and environmental characteristics. They finally suggested the basic principle to success is to integrate multifaceted prevention-intervention programs with specific community settings.
The aim of this thesis is to review the problem of adolescent drug use about volume of the problem (epidemiology), risk and protective factors, and etiology focusing on Lake County, Oregon as a frontier community. The researcher will expand the scope of adolescent substance use providing a brief outlook on various societal dimensions and different strategies for prevention and control of adolescent substance use. In addition, the thesis aims to provide a preliminary assessment of the efficacy of Dr. Gil Botvin’s Life Skills Training Program for the middle schools’ student population of Oregon.
Specifically as applied to the 6th and 7th grade student population of Lake County Oregon as a frontier community during the years of 1998 through 2000. The researcher displays a personal experience working on Botvin’s Life Skills training program for prevention of adolescent substance use in a frontier community (Lake County, Oregon) and will provide a detailed analysis of the work done in Lake County and interpret these results to examine the applicability of Botvin’s Life Skills in a frontier community.
Definitions
On reviewing the literature on adolescent substance use, there is little agreement to the terms that point to various patterns of drug use. Terms of substance or drug use, abuse, and dependence are erratically used instead of one another. For this thesis’ purposes of discussion a drug definition is as suggested by Fagg (2006). A drug is a psychoactive substance that acts on the central nervous system influencing the mood, behavior and thought (Fagg, 2006).
Drug use definition is as in the WHO (World Health Organization) expert committee report on drug dependence (2003). A substance use is the intentional taking in of a substance that influences the individual’s behavior, way of thinking, feelings, or insight. Figure (2) shows licit and illicit substance use among US adolescents in 2008 based on data of the National Survey on Drug Use and Health (SAMHSA), 2007 (Dawes and others, 2008).
According to Australian Statement of Principles concerning drug dependence and drug abuse No. 16 of 2008, this substance (drug) should not result in habituation (psychological indigence), or addiction (physiological indigence). The individual is always capable to control the amount used. Finally, this substance should not result in extraordinary effects on the individual’s mental, physical health, and life functioning (work or social).
Based on the definitions cited in the Australian Statement of Principles No. 16 of 2008, the definition related to drug abuse is. A psychiatric state fulfills the following. It should be a poorly adapted pattern (prototype) associated with drug use resulting in a notable afflict or harm. The individual shows one or more of the following criteria within 12 months of drug use. Repeated drug use results in failure to fulfill a principal commitment (work, school, social, or family). The individual does not refrain from using the drug in possibly risky situations as driving or working on a machine. Other signs include repeated use of the drug despite exposure to legal problems, social or family problems caused by, or aggravated by using the drug.
Drug dependence is the psychiatric state that fulfills at least three (or more) of the following signs on condition, they take place within 12 months of drug intake. First is the tolerance, it takes one of two forms, second , either there is a need to take increasing doses to get the wanted effect or continued intake of the same dose results in reduced effect. Third, drug withdrawal results in symptoms relieved by drug intake.
Fourth, is despite continuous urge to stop the drugs but repeated trials persistently failed. Fifth, longtime, persistent, repeated and failing efforts spent trying to control of the drug intake are signs of drug dependence. Other signs are reduction or missing significant activities whether social, work related, leisure related, because of the individual keeps on taking the drug (Australian Statement of Principles concerning drug dependence and drug abuse No. 16 of 2008).
A frontier community definition, as stated by the National Center for Frontiers Communities (2000) is a community with a population density of less than, or up to 20 persons per square mile. It should be located at a great distance or travel time from the nearest sizable service center (education, or medical) or market.
However, this definition does not consider the population characteristics as senior population, income, or health conditions. Nor does it consider whether service centers and markets are within the state borders or not. Therefore, the National Center for Frontiers Communities recommended that states should take part in both defining and designing a frontier community. According to this definition, nine million US citizens live in frontiers communities, twenty-seven states have 97 counties to consider as frontiers communities (The National Center for Frontiers Communities, 2000).
In 2003, the United States Congress passed the public law 107-251 assigning the Secretary of Health and Human Services to define what a frontier area is. The definition bases were mainly population density, and travel distance to the nearest medical facility. The expert panel assigned to examine the definition suggested that frontier areas are those zip code areas fulfilling the following conditions. They should be 60 miles or more far from a nonfederal hospital of at least 75 beds along the fastest paved road. Alternatively, an area on 60 minutes travel time from a similar health facility is a frontier area. Finally, a frontier area should not be a part of a larger rural town of 20000 inhabitants (Center of Rural Health at the University of North Dakota, 2006).
Dimensions of community
A community is a construct (a structure or a model) and it is not just the people living in. Defining a community in sociological terms, it is a social model where its members have a common array of shared interactions, and behaviors, which have a common meaning and prospects. Communities are dynamic builds since interactions, and mobilization link communities irrespective of size, facilities, or economic differences.
In urban areas, there are multiple communities based on two main factors, first is the ethnic, linguistic, or religious heterogenicity of the population, second is the mobilization from rural and suburban communities for better economic, or technological opportunities. The factors may account for the sociological differences between urban, rural and frontiers communities. The use of the word dimension instead of parts (for example) implies that we look at analytical categories and not observable parts of the community. One method of analysis is to look at differences or diversities that break a community into categories (Bartle, 2007).
Cultural diversity and adolescent substance use prevention
Adolescent substance use prevention is a message and like any other message it has to adapt to situation, audience, other communicators, context and topic. Since effectiveness remains the main objective of any prevention program, there are two arguments about the way to impose such programs. First is to set up a universal program, but most researchers; however, favor imposing programs with the potential of modification to suit local communities’ culture assuming this provides maximum program effects (Hecht and Krieger, 2006).
Schools are the natural primary site to deliver adolescent substance use prevention programs. In elementary and middle schools most children and adolescents can be reached whereas in high schools dropout is an obstacle to reaching target audience. Therefore, preventive programs have to acknowledge that schools reflect the cultural as well as other facets of diversity in the US society (Hecht and Krieger, 2006).
Elliot and Mihalic (2004) reported most teachers consider cultural diversity a limitation in applying most substance abuse prevention programs, and hold themselves responsible for adapting the programs to meet the students’ diversity. Thus culture base of a prevention program is the foundation of a successful prevention message. However, standardization of the type and extent of modifying the prevention program are important considerations to look at.
The communication accommodation theory provides a theoretical viewpoint to support cultural adaptation of prevention programs. The theory explains how diversity works in an interpersonal background and argues that interpersonal cultural diversity influence interaction among people. The theory puts forward three possible mechanisms for cultural adaptation, first is maintenance where communicators observe the difference and maintain its level. Second mechanism is divergence, which occurs on rejection others’ identities then the communication pattern has to change. Third is convergence, where modification pattern may result in under or over modification either is a relevant issue of the effectiveness of the prevention message (Gallois and others, 2005).
Resnicow and colleagues (2000) defined cultural sensitivity of a prevention message as the level cultural characteristics of a target population are integrated in a prevention program. They defined cultural competency as the ability of individual (mainly practitioners) to practice interpersonal cultural sensitivity. Culturally designed preventions and intervention are those adapted to the cultural characteristics of the community, and culturally based prevention programs are those using cultural characteristics to stimulate behavioral changes (Resnicow and others, 2000).
Generational diversity and adolescent substance use
Addressing the needs and differences of age groups is important to harvest the benefits of whatever policy, prevention program or organizational performance. Research pointed to age as an important deciding factor for needs, values and extent of accepting sociocultural norms and that members of each group have separate arrays of values, attitudes, and behaviors (Columbia, 2005).
Adolescents represent a vulnerable age group because of the rapid biological changes, remarkable individual variation, and growing to developmental and cognitive maturity. Other distinctive features are lack of feeling of authority, and dependence on adults for taking informed decisions.
Thus, the principle of (one size fits all) is not suitable when planning healthcare or prevention programs for adolescents. On the other hand, adults (researchers, family, or communicators) must be aware, responsible and share decision making with adolescents (Gullotta et al, 2005). Researchers recognized two phases of adolescence early and late, the limiting age varies as the classification depends on the rate of developmental and cognitive growth. The differences between the two phases are the degree of attention to adults, parent-adolescent relationship, the cognitive processes leading to decision making, degree of attention to reciprocal relationships. It is noticeable that media particularly television use is greater in early adolescence (Gullotta et al, 2005).
The first question should prevention programs be designed specifically or modified to meet the characteristics of younger or elder adolescents. Williams and colleagues (2002) argued that a theoretically reliable and effective health psychology research for prevention or treatment should be based on a developmental outline. They inferred that adolescent’s prevention intervention programs must be specifically designed, highlighting that in this stage adolescent establish their lifelong configuration of self-management and adjustment. They suggested a three steps prevention programs design for adolescents, primary prevention aiming at modifying risk factors before the onset of the disorder.
Secondary prevention should aim at early identification and intervention to abort the problem before progressing to a major one, in terms of substance use, secondary prevention should prevent the progression to abuse or addiction. Tertiary prevention centers on preventing conditions that may result in lasting or irreversible damage as moving to illicit drugs or associated health hazards to substance use (Williams and others, 2002). About intervention, Kaminer (2005) showed that group intervention particularly if including adolescent with problem behavior can produce iatrogenic effects on all participants because of heterogenicity. Kaminer (2005) inferred that to enhance group intervention an attention to preventing, reducing, and controlling such iatrogenic effects in heterogeneous groups should be made.
The second question would be do age differences between parents or teachers and adolescents minimize their role on prevention so to give peers a leadership role than adults. Cuijpers (2002) responded to the hypothesis that peer led substance abuse prevention programs are more successful than adult led school drug prevention programs conducting a meta analysis of the studies compared results of both categories.
Cuijpers (2002) noticed that results differ variably from minimal to significant differences; however, the author concluded that this variation of results is because leadership constitutes one factor among other factors that determine prevention program effectiveness. Wood and colleagues (2004) examined the peer variables (alcohol offers, modeling, and perceived norms) compared to parents’ (monitoring, values, and attitudes) in a group of (556) late adolescents on alcohol use. Stratified regression analysis of questionnaires results showed that both peers and parents influence alcohol use, however, higher levels of parent-adolescent involvement link to weaker peer influence. They inferred that parents can still exercise an influential role in late adolescents drinking behavior.
Gender diversity and adolescent substance use
Over the past few years, research showed there are differences between male and female substance use and abuse. Spooner (1999) suggested the age of initiation of alcohol use in males is less than that in females, further; males tend to drink heavier and experience more alcohol related problems than females. The National Institute on Drug Abuse suggested these differences have an impact on drug abuse and progression to dependence; moreover, the differences should have an impact on prevention programs and intervention modalities (NIDA, 2000). The explanation was that males have a greater opportunity to use drugs; however, NIDA research showed that tendency differs, whereas males are abusers to alcohol and marijuana, females are more abusers to sedatives. Other social factors that contribute to this difference were females’ increased rates of education drop out and lesser employment rates (NIDA, 2000).
Thus, the problem of drug abuse in females can be looked upon separately as female adolescent substance abuse syndrome (Dakof, 2000). In addition, Dakof (2000) inferred males and females referred to treatment present different clinical features of drug abuse. Lynch and colleagues (2002) looked into the biological basis of male and females tendency differences of drug abuse and inferred that evidence suggests there are differences in biological response to drugs, long-term effects, causes, and correlates of drug abuse.
Low enforcement as a diverse culture
Many adolescent substance prevention programs include law enforcement concept, thus understanding low enforcement as a culture may highlight evaluation of different programs. Shusta and colleagues (2008) recognized lack of trust between police and society as a whole as a community sub culture. They identified the attitude of some police officers as a cause of encouragement for this distrust; further because of distrust, police members look to each other for primary support. Shusta and colleagues (2008) suggested that police officers tend to develop their own culture affected by the work stresses and anxiety.
Adding this to their tendency to interpret behavior, motivation, and illegal activity from their cultural point of view creates controversial viewpoints about interpretation of law and its enforcement. In the lights of the diversity of the society, this creates a challenge in law enforcement (Shusta et al, 2008).
Dent and colleagues (2005) examined the level of availability of alcohol in 92 Oregon state communities in relation to enforcement laws as predictors of adolescent alcohol use. Thus, they examined the link between strategies of restricting access and enforcement of possession laws on adolescents alcohol use. There were four outcome measures examined, frequency of alcohol use within 30 days of the study, use of alcohol at school, binge drinking, and drinking and driving.
Their results displayed a correlation between all four outcome measures and the rate of illegal alcohol sales. Besides, the level of enforcement of possession influenced significantly the rate of expansion or contraction of using different sources of alcohol sales in a community. Although they recognized that data are epidemiological in nature based on observation from questionnaire sheets subjected to individual and societal variation, yet, they inferred there is experiential support for efforts to control alcohol under age sales and possession enforcement.
Summary on social epidemiology of adolescent substance use
Adolescent substance use is in the center of interest of any academic specialties (sociology, epidemiology, psychology and public health); research suggested that no single discipline can explain the causes, risk behavior, or outcomes of the problem. Social epidemiology focuses on the social factors that characterize the population distribution of substance use behavior. Socio-epidemiological research is defective in evaluating the link between background variables like neighborhood socio-economic conditions, isolation, discrimination and adolescent substance use. In addition research suggests that endogenous factors (genetic or biological) alone cannot be held responsible for causing the problem. It is the combination between exogenous (social, economic, or educational) and the endogenous factors that shape adolescents’ risk behavior for substance use and abuse (Galea et al, 2004).
Epidemiology of substance abuse
Evelyn and McKnight (2007) (Brain Institute Report) stated that in 2001, 1.9 million US adolescents (between 12 and 20 years) were heavy alcohol drinkers. The cutoff point is 14 drinks a week or 4-5 drink at a sitting for males and female heavy drinkers were those who had seven drinks a week or three drinks at a sitting. While 4.4 million were not heavy but overdo drinkers. The problem is not a US problem solely, Evelyn and McKnight (2007), reviewed UK, and Brazilian epidemiological studies and inferred that in UK, 20% of adolescents at 12-13 years consume alcohol. The rate rises with increasing age to reach 50% by the age 14-15, and 70% at the age of 17. In Brazil about 90% of students between 8th to 11th grades reported trying alcohol.
Klein, Shane, and Barry (2003) reviewed the results of 2002 National Survey on Health. They pointed to more than 17% of adolescents aged 12-17 years included in the sample reported drinking alcohol once during the last 30 days before the survey. Over ten percent of the sample’s adolescents reported, overdo drinking, and another 2% reported heavy drinking. About illicit drugs, 11.6% of adolescent included in the survey reported using illicit drugs at least once during the last 30 days before the survey.
Over eight percent reported marijuana and 5.7% reported methamphetamine or other drugs. There were no significant differences between males and females about alcohol or illicit drugs use. Twelve percent of eighth grade adolescents reported drinking alcohol at least once in the last two weeks before the survey. More than three percent of 12th grade adolescents reported drinking alcohol daily for the past month before the survey. For illicit drugs, 10.4% of 8th grade adolescents reported illicit drug use in the last month before the survey. The survey also showed that 21.5% of 12th grade adolescents reported using marijuana at least once in the last month before the survey.
Overall 6% of adolescents included in the survey sample used marijuana on daily basis during the last month. Klein and colleagues (2003) reported that black adolescents used alcohol less than white and Hispanic (23.7%, 50.4%, and 49.2% respectively). Further, 13.3% of adolescent included in the survey reported driving after drinking alcohol, and 31% reported being with someone driving after drinking alcohol at least once in the month before the survey (Klein and colleagues 2003).
In 2006, the National Survey on Drug Use and Health displayed that 25% of adolescents between 12-20 years were current alcohol consumers. Besides, 20% drove under the influence of alcohol in the last 12 months before the survey. Further, the survey showed that 1900 deaths under 21 years take place yearly in car accidents under the influence of alcohol. The survey showed that 30.3% of adolescent included drank alcohol in their homes. More than ten percent of males drank in a club or a restaurant compared to 20% of females included. The report called to increase parent mentoring and to readjust current prevention tools (The NSDUH Report, 2008).
Although drug use varies among frontier, rural, suburban, and urban communities, yet some characteristics of frontier communities make the depiction taken. These features are poverty, as 50 of the poorest counties in the US are frontier counties, adolescent under 18 years represent 26.7% of the population (compared to 25.7% in other areas of the US).
Opposite to public perception and to the picture drawn by the media, adolescent in frontier communities are at similar or even greater risk of drug use. They are prone to the same stresses and persuasions as their counterparts all over the US. In addition, frontier counties’ adolescent have lower rates of finishing school study and attending colleges (The National Clearinghouse for Frontier Communities, 2003).
Based on the report of the National Clearinghouse for Frontier Communities, 2003, alcohol use by frontier communities’ student is similar to their counterparts all over the US. In addition, as it is the case all over the US, alcohol drinking and tobacco smoking dominates over illicit drugs use. The association between drinking and driving is higher in adolescents of frontier communities. This is because of lesser means of entertainment, and greater distances to the nearest activity centers. Particular to frontier communities with large population of Indian Americans and Alaska natives is the higher rate of illicit drugs use, 23% of these adolescents between 12-17 years used illicit drugs.
Drug use on regular basis is of smaller rates among adolescents in frontier communities. Forty eight percent of adolescents who smoke are prone to use illicit drugs compared to 5.3% of nonsmokers. Further, 65.3% of adolescents who drink alcohol are prone to illicit drugs use compared to 5.1% of non alcohol users (The National Clearinghouse for Frontier Communities, 2003).
Volume of the problem
Brain Institute, University of Florida (2007) reported that in 2001, 1.9 million adolescents between 12-17 years were heavy drinkers (<14 drinks a week or 4-5 drinks per setting for males, and 7 drinks a week or 2-3 drinks per setting). Binge drinkers (< 5drinks a setting) in the same age group were 4.4 million and underage alcohol users are 20% of alcohol consumers across the US. Among 9th To 12th grade adolescents, 75% had at least one drink in the last month. In 2003 the National Survey on drug use and health reported that binge drinking rates were 0.9% among adolescents at age 12 years. At 13 years, it was 2.2% at, 7.1% at 14 years and escalating to reach almost one fourth of adolescents at 17 years. In 2004, the Future Monitoring Survey reported that rate of alcohol among adolescents nationwide did not change from the previous survey in 2003 (Evelyn and McKnight 2007).
In 2008, the National Survey on Drug Use and Health reported that (in 2007) tobacco use among adolescents decreased compared to 2002 results regarding cigarette smoking, but smokeless tobacco rate increased in the same period. In 2007, 1.8% of adolescents between 12 to 13 years were cigarette smokers, between 14 and 15 years, 8.4% of adolescents were cigarette smokers, the rate escalate to reach 18.9% of adolescents between 16 and 17 years. In the same report, the rate of illicit drug use among adolescents aged 12 to 13 years was 3.3% rising to 8.9% at 14 to 15 years, and 16% among 16 to 17 years adolescents. The report shows that the ratio of those whose first illicit drug used was a tranquilizer increased from 2.4% (in 2002) to 6.5% in 2007 (Office of Applied Studies, 2008).
The US frontier community extends over half the land area of the US with population less than 4% of the total US population. Despite that, frontier population is poorer (the poorest 50 US counties are frontiers), depending more on agriculture, and less medically insured. Frontiers adolescents are subjected to the same stresses and temptations as their counterparts in urban areas. The US Census bureau uses the term metropolitan and non-metropolitan areas, however, many researchers use other terms to define frontiers (like population density less than 1000/ square mile) (Frontier Education Center, 2003).
Data collected by the American Drug and Alcohol survey and Prevention planning survey on 7th, 8th, 11th, and 12th grade adolescent in nine rural communities showed adolescents living in frontier area to small cities are equally influenced by alcohol and other substances. Exogenous risk factors like family conflicts, having friends who are drug users (peer effect) appear to influence rural and frontier adolescents in these areas and are positively correlated to alcohol use.
In addition, economic uncertainty and changes in social patterns and community interconnection were important factors. Among the relevant endogenous factors poor adjustment to school, and depression and the need for excitement (for females) were the most common (Frontier Education Center, 2003). However, the report acknowledged that generalization on rural and frontier adolescents’ trends of substance use cannot be drawn from these results as the rates differ among individual rural or frontier communities (Frontier Education Center, 2003).
Risk and protective factors for adolescents substance abuse
An understanding of the changes that occur during adolescence and the theories of adolescent substance use should explain risk and protective factors specific to this age group. Behavioral changes in response to re-adjustment, new stresses and anxieties characterize adolescence; it is a period when identity is established in preparation to practice new roles in life. During this stage, practicing adults’ behavior shifts from play to actual behavior and dependence on parents decreases while reliance on peers increases. Another characteristic of adolescence is the increased tendency to take risks either for experimentation or excitation. There are three basic theories that may explain adolescent substance use (Langrod and others, 2004).
Theoretical backgrounds
Social learning theory
The basic elements of this theory are adolescents learn through sensationalist observation of role models behavior and the outcome of this behavior. Thus, role models help adolescents to shape their beliefs about what is normal, popular, or acceptable behavior. However, personal factors like knowledge, personality, skills, and aims may alter adolescents’ vulnerability to role models effects. The theory, therefore, highlight the importance of self-regulatory mechanisms to alter role model effects. Role models can be parents, peers, or siblings where elder peers and siblings play a more important role and are high-status role models (Langrod and others, 2004).
Problem behavior theory
This theory recognizes that behaviors acceptable for adults as age specific but prohibited for adolescents are considered as signs of shifting to maturity. Such a behavior may help adolescents to achieve certain aims like impressing their peers or coping anxiety or failure. Thus according to this theory, substance use is functional or is an instrument to achieve certain objectives. The main problem is if such a behavior succeeds in achieving an aim (as impressing peers); it is difficult to put it out without finding an alternative (Langrod and others, 2004).
Kim and others (1995) inferred that unless adolescents learn alternative ways to achieve their aims, substance use may be impossible to modify results of intervention prevention programs. Looking at both theories, there is noticeable complex multiplicity of risk factors contributing to adolescents’ substance use problem, and that they can change through stages of adolescent development. Besides, it is difficult to decide the mechanism of interaction of risk factors ending up with substance use problem (Beman, 1995).
Social identity theory
This theory provides a slightly different viewpoint on social influences that centers on the adolescent’s self-conception as a member of a group and the classification of different social groups. Based on this theory, an adolescent self-conception is a mixture of various self-images that follow a scale of images from (as an example I drink beer) to (I am a member or belong to a group that drink alcohol). The degree where an adolescent social identity takes the priority in a given situation is decisive in shaping the risk behavior. Further, adolescents integrate their social identity to the group’s identity (Kobus, 2003).
Risk and protective factors to adolescents substance abuse
Awareness of risk and protective factors besides reducing risk and enrichment of protective factors (encouraging buoyancy or resilience) are the center of any prevention program (Office of Drug Control Policy (b), 2002). Based on the Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking Report (2007), a risk factor is the quality, characteristic, or vulnerability factor. This factor makes an individual more prone to develop a disorder more than a randomly selected individual from the general population.
Risk factors should, therefore, precede the onset of the disorder; they are dynamic, which means they are changeable because of individual’s development or a newly evolving stressor in an individual’s life. Risk factors assigned to the individual, family, society or institution (work, education, prison…). Risk factors can be unchanging, like gender or family history or altered by interventions, like education level or exposure to maltreatment. Protective factors are those which improve an individual’s response to a stressor, in other words they produce a better adaptive adjustment and influence the response to risk factors.
Buoyancy or resilience construction correlate more to protective factors, as well to the individual’s competence to withstand a stress or recover from psychological trauma induced by others. Recognizing risk factors is essential to identify populations where intervention is likely to produce best results. Thus prevention depends on marking risk factors that are more compliant to alter by intervention, and seeking out protective factors to augment and improve (the Surgeon General’s Call to Action to Prevent and Reduce Underage Drinking, 2007).
Beman (1995) recognized risk factors that make adolescents more vulnerable to drug use and abuse. They are population’s characteristics (demographic), collective communal, behavioral, and individual risk factors. Wright and Pemberton (2004) summarized the risk and protective factors for drug use in adolescents as follows, based on data taken from the 1999 National Household Survey on Drug Abuse.
Factors related to community
The survey showed that adult neighbors strongly disapprove their neighbor adolescent smoking cigarettes daily, drank alcohol daily, or tried marijuana. Ratios ranged between 75% and 65% and were highest on trying marijuana, and lowest on daily smoking. Easy getting hold of marijuana reported by 57% of adolescents, and there was no difference between White, Hispanic and Black adolescents. However, White adolescents reported more local community orderliness and less ineptitude (Wright and Pemberton, 2004).
Family related factors
Most parents disapprove their children smoking cigarettes, drinking alcohol or trying marijuana. Rates ranged between 95% for trying marijuana, to 85% on smoking cigarettes. Fifty seven percent of adolescents reported they have had a conversation, at least once, with one of their parents on the hazards of drug use during the 12 months before the survey. Whites and Hispanics reported parent communication on the subject more than Black counterparts. About parent mentoring, 81% of adolescents reported parents’ help in homework, but 39% reported parents limiting TV watching time (Wright and Pemberton, 2004).
Factors of the individual realm
Almost two thirds of the adolescents included in the survey (64%) reported they would strongly disapprove their counterparts trying marijuana. On the other hand nearly the same rate (63%) reported their friends would strongly disapprove them trying marijuana, repeatedly drinking alcohol or heavily smoking. Most adolescents included (57%) reported they realize the hazards of smoking marijuana even once or twice a week.
About religious beliefs, the survey results displayed that 80% of adolescent think that religious belief is an important part of their lives, and 74% reported they influenced their decision in various sides of life. Further 37% reported that their friends share the same concepts about religious beliefs. Male adolescents reported less appreciation of the hazards of substance use and abuse than female counterparts. Adolescents aged 15-17 years showed higher perception and more positive outlook to substance use than their 12-14 years counterparts. About aggressiveness, 22% of adolescents included in the survey reported they had a serious fight whether at school or workplace during the last 12 months before the survey. Interestingly, 8% reported they attacked someone intending to induce injury during the same period (Wright and Pemberton, 2004).
School factors related to substance use
Most adolescents included in the study reported they would have serious troubles in schools if found using marijuana, drinking alcohol, or smoking with rates of 95%, 86%, and 63% respectively. Despite that, 23 % of adolescents reported their friends in the school have used marijuana at least once. On the bright side, 77% of adolescent reported receiving at least one school notice about hazards of substance use. White adolescent reported lesser bond to school rules than their Hispanic or Black counterparts (Wright and Pemberton, 2004).
Wright and Pemberton (2004) inferred that after adjusting the variables of age, gender, ethnicity, and community demographic differences, there is a strong association between risk and protective factors. Prevention message from the school and church have strong influences on adolescents. Also, parental communication, mentoring, stronger controls on substance use in school have strong influences on adolescents about substance use. Table (1) summarizes the risk factors for adolescent drug abuse among other psychosocial phenomena (Catalano and Hawkins, 1996).
Risk and protective factors to adolescents substance abuse in frontier communities
The 2003 report of the National Clearinghouse for Frontier Communities points to the following key issues about specific risk and protective factor for substance use in frontier adolescents. The literature researching high risk behavior in frontier adolescents is deficient. It also overlooks specific issues of risk and protective factors to drug use in frontier adolescents. The report included data on rural areas’ adolescents in many areas where data on frontiers adolescents are not available.
The report pointed to the relationship between poverty and serious emotional disturbances among frontier’s adolescents which may lead to substance abuse. The report also represented the lack of trust of frontier’s adolescents in health professionals to discuss their problems and assigned this to frequent turnover of health professionals in these communities.
Frontier communities’ poverty and behavioral health problems reflect on the family life of these adolescents. Besides, gun carrying being more acceptable in these communities and rural ones marks the problem of increased societal hazards of drug use. Finally the report associates violence and drug use irrespective of the degree of drug use involvement. Another area where specific data on frontier communities are deficient is the education dropout rate.
Although data suggest slight differences between rural, frontier, and urban education dropout rates, however, return to education after dropping out is higher in urban and suburban communities than others. Many expect schools in frontier communities to provide an individualized mentoring and guidance than those of urban communities. However, the trend of combining schools into a single education mass (school consolidation) disrupted this advantage (the National Clearinghouse for Frontier Communities, 2003).
Summary on Adolescents substance abuse risk factors
Adolescent substance abuse risk factors are four main groupings. First are cognitive and personal attitudinal risk factors, which are centered on awareness of the negative outcomes of substance use, they link to personal capabilities and decision making competency (Griffin and others, 2001). Second is personality factors, Sussman and colleagues (2002) reported many personality disorders correlated to adolescents’ substance use like low self-esteem, low social and self-confidence. These adolescents are characteristically impetuous, insubordinate, and more anxious; however there is common characteristic personality pattern to describe them (Sussman et al, 2002).
Further, many research studies link personality and psychiatric morbidity to substance use and establish a significant link between the development of conduct behavioral disorders and substance use (Langrod and others, 2004). Third are sociocultural factors, family attitudes, behavior, and management style are strong influential factors that correlate positively to adolescents substance use. Parents’ attitudes (tolerance) to substance use, the quality of parents-adolescent relationship, lack of involvement in adolescents, activities, and use of guilt feeling as a motivation are all blamed for substance use. Many researchers believe that peer effect is stronger especially at the adolescent stage of development, specifically in initiating experimentation, and providing support for use particularly if adolescents are involved in social networks.
Other social factors to consider are socioeconomic level and work involvement during school study (Langrod and others, 2004). Since cultural values are reflected in family and community consistency, supervision, and monitoring of adolescent behavior and relationships, thus, they affect initiation and the course of adolescent substance use. The society look to ethnic diversity has a considerable effect on the risk of minority adolescent substance use (Langrod and others, 2004).
Genetic influence on adolescent substance use is evident from studies on monozygotic, bi-zygotic, and adopted twins. Also studies shows that adolescent with positive family history of substance use are at higher risk to develop substance use. Biological markers associated with high risk include alcohol dehydrogenase deficiency (common in Asians), and reduced amplitude of certain waves (P3 wave) in evoked response neurological testing (Langrod and others, 2004).
Summary on Adolescents substance abuse protective factors
Research on protective factors received less research attention, family religious culture mediated to adolescent represent a strong protective factor. In addition, emotional support to adolescents through open parent-adolescent communication style, and flexible monitoring of peer activities are protective techniques. Involvement in organized school activities and school academic achievements are also protective factors (Langrod and others, 2004).
As indicated in the report of the Frontier Education Center (2003), there is scarcity of research on risk and protective factors influencing frontiers adolescents. And most research studies focus on American Indians and Alaska natives who have particular sociocultural environment. Thus, conclusions about adolescents’ risk and protective factors made from these studies are not applicable to all frontiers adolescent (Hawkins and others, 2004).
Factors affecting relapse of substance abuse
Relapse to substance use or abuse is the event of returning to drug abuse and is a process that takes place over a period of time. It is more common with drug addiction or dependence than with drug use, and it is the result of failed intervention or treatment. Thus, relapse rates depend on the type of intervention or treatment directed to an adolescent, the method of detecting relapse. The main causes are genetic and biological, persistence of stressful socioeconomic factors, unhealthy peer effect, or failure of protective family environment. Theoretical explanation of relapse can be in both social learning theory, and problem behavior theories (Tims and Leukefeld, 1986).
Relapse prevention is currently based on the cognitive behavioral hypothesis, which is in the domain of psychologists (Witkiewitz and Marlatt, 2004). However, since relapse is an individual’s return to substance use it is different in that further research needs to focus on the impact of socioeconomic factors on a particular adolescent trait more prone to relapse. Besides, the mechanism of interaction between sociocultural factors and genetic or biological factors needs further study (Galea and others, 2004).
Etiology of adolescents substance abuse
Etiology is to describe a disorder’s causes. It reflects the scientific research into the disorders’ origin on biological, psychological, or socio-cultural basis. What adds to the etiology complexity of a disorder is often the presence of a combination of many causes. An understanding of the causes is important for effective treatment and specific for psychology, a comprehensive understanding is critical for behavior modification (Benner and Hill, 1999).
In exploring the huge landscape of gathered data about the etiology or casual factors of adolescent substance use, the factors responsible for inappropriate substance behaviors are complex and multifaceted. The processes and interactions of various factors which may predispose or lead an adolescent to engage in substance use are ambiguous. For the sake of briefness, the four basic approaches of research into understanding the etiology of substance use and misuse will be reviewed. These four considerations are the biological-genetic, the psychological, the psychosocial, and the sociocultural considerations.
The biological-genetic considerations
One major part of the biological research has postulated a theory which suggests the genetic or hereditary familial transmission of alcoholism (Cotton, 1979, Goodwin 1986, Dawson, Harford, and Grant 1992). The theory is based mainly on the high correlation found between the incidences of alcoholism among the offspring of known alcoholics. The research interpretations signal that biological sons of alcoholics are four times more likely to become alcoholics than those sons whose biological fathers were not alcoholics (Goodwin 1984). The twin studies conducted in Sweden and Finland, and the adoption studies in Denmark beginning in the 1970’s support such a view.
The data from the twin studies displayed a higher evidence of alcoholism among identical twins than non identical twins. The results of the adoption studies further underscored the validity of the theory of genetic transmission. It was found that biological sons of alcoholic fathers, adopted in the first few weeks after their birth, were still four times more likely to develop alcoholism regardless of who raised them (Monteiro and Schuckit, 1988).
Based on this study, a further distinction can be made, suggesting a clear outline between familial transmission, and the possible impact of environmental factors. The eventual alcoholism syndrome appears uninfluenced by the environment of the substitute family as shown with adopted sons (Goodwin 1986). Although the data suggests a strong genetic factor, it is significant to note how genes are transmitted and how environmental factors interact with inborn traits to cause the disorder is not yet known. It is also noteworthy that purely genetic factors cannot fully explain the etiology (Gordon and Glantz, 1996).
The second major part of biological research into the etiology of substance use focuses on specific organs or organ systems. Research endeavors to find out the genetically programmed effects mediating or influencing biological functioning are not yet complete. Researchers have suggested that genetic origins have affected some functions in such a way to influence individuals having certain vulnerabilities or tendencies to develop substance abuse (Schuckit and Smith1996). The effects of low levels of aldehyde dehydrogenase, and the responsiveness to the chemical neurotransmitter serotonin are examples of the factors considered as probable influences to develop a tendency to alcoholism (Schuckit 1994).
The principal hypothesis of biological and genetic etiology for drug use is parent transfer genetic tendency to substance use to their children. It shows in adolescent temperament, brain response to different doses whether large or small, and susceptibility to unfavorable outcomes (Sheckter, 2000). Silberg and colleagues (2003) examined genetic and environmental inclination to substance use; their results showed that genetic transmission was more prevalent in female adolescents with substance use.
Genetic factors were also important in the association between substance use, conduct disturbance and depression in female adolescents. Environmental factors evinced by family failure to provide a healthy environment and abnormal company influenced adolescent males more than genetic factors. However, about association of substance use, conduct disturbance, and depression genetic factors played a role, but environmental factors were dominant.
Spear (2002) reviewed the biological basis of brain development in adolescents and the influence of neural changes on the tendency of alcohol use and abuse. Spear (2002) suggested the main characteristics of adolescent brain are developmental changes of the prefrontal cortex, stressor sensitive areas in the forebrain that are dopamine dependent. These areas are part of the neural network responsible for adjusting the incentives for alcohol use. Another characteristic suggested by Spear (2002) was adolescent brain shows signs of augmented stressor reaction. Of equal importance adolescent brain shows modified sensitivity to alcohol effects. The author inferred there is a need for further studies to examine if alcohol use during adolescence results in disturbing maturation of alcohol sensitive brain areas.
The Psychological considerations
Psychological factors influencing substance use in adolescents refer to the models and patterns of thinking and behavior. Examples are personality characteristics, self-image, and adjustment skills (Deas and Thomas, 2002). Sheckter (2000) reviewed the various psychological theories that influence adolescent risk to develop substance use problem, these are:
Considerations on self-image, social-image, and self-disparagement (derogation)
Adolescent self-image and social image about substance use mainly smoking and alcohol drinking are affected by three factors, first is the consistency factor, which is self-ideas and concepts are consistently related to the substance used (consistency hypothesis). Second, is whether adolescents’ ideal self-image relates to the substance use, this is the self-enhancement hypothesis that is improving one’s image or adding strength, worthiness or a desirable characteristic. Third, is whether substance use impresses friends, and this is the impression management hypothesis (Chassin and others, 1985). Chassin and other (1985) analyzed the drinking behavior in 266 adolescents in a suburban high school and inferred alcohol drinking behavior follows both consistency and self-enhancement theories. They also inferred that male adolescents’ intent to continue drinking alcohol relates to consistency and impression management theories, while adolescents’ females intents relates to neither of these theories.
Self-disparagement (derogation) hypothesis correlates to self-confidence (self-esteem) reasoning. This means the personal need of augmenting positive self-attitude skills or knowledge (Sheckter, 2000).
Personality hypothesizes
They consider substance abuse a display of a personality disorder. In Freud scholars’ terms, substance abuse reflects a passive, dependent personality, which suffers oral frustration (expression of explanation). In mid 1950s, the domain of personality disorders became important in identifying users. In this framework, the Minnesota Multiphasic Personality Inventory, 1969 represents a cornerstone. Based on this inventory, there are five personality traits related to substance use, insubordinate, feeling inferiority leading to passive belligerence, chronically distressed personality, and demanding personality (Sheckter, 2000).
Tension lessening hypothesis
Based on this hypothesis, states like stress and anxiety give reason to act aggressively. Such conditions can be an enough steer for substance use and abuse (Sheckter, 2000).
The psychosocial considerations
Lee and colleagues (2004) suggested that social learning is the main psychosocial theory that determines adolescents’ drug use among other unacceptable behaviors. The central hypothesis of this theory is development of behavior takes place through observation and underpinning. In other words an individual learns new behaviors by watching a model presentation, be present at the onset, and is impressed by the behavior to reproduce it.
Sheckter (2000) explains this theory’ influence on adolescent substance use, not only about picking up the habit of substance use but also in picking up the behavior and conduct associated by mimicking those accompanying in the primary involvement. Social learning theory has two principal constituents (as suggested by Sheckter (2000), self-efficacy and expectancies. Self-efficacy is connected to individual expert skill and complete self-control. Expectancies explain the most probable results accompanying a certain behavior. Sheckter (2000) described a practical example, if Y watched X having few drinks then successfully asked a young woman for a date, then if Y drinks alcohol it may improve the chances for similar successful results.
The second hypothesis is the social control theory first described by Hirschi (1969) (after Sheckter (2000). The hypothesis assumes that unfavorable adolescents’ behavior is not an eccentric abnormality. Alternatively it is an inherent trait of adolescents. In this sense, unfavorable adolescent behavior does not merit explaining and efforts should be directed to explain its consistency. Based on Hirschi’s hypothesis conventionality or consistency of such a behavior comes from attachment, commitment, involvement, and belief (Sheckter, 2000).
Third is the reputation enhancement hypothesis. The key assumption of this hypothesis is that adolescents choose the social distinctive image they want to promote in their community. The key percept is that defining a unique identity for an adolescent depends on persuading others to define him or her in the way an adolescent wishes. The essential tools to achieve this are the alternatives an adolescent considers, descriptions and details and justifications given (Sheckter, 2000).
Fourth is the problem-behavior hypothesis. It is the behavior that is far from accepted socially and legally and is disapproved by members of society and institutional authorities. The principal objectives of this hypothesis are three shared socio-psychological prominent schemes, the personality scheme, the behavior scheme, and the recognized environment scheme (Sheckter, 2000). These schemes interact to produce susceptibility to problem behavior (Sheckter, 2000).
Morton (2007) examined the eventual relationship between adolescents and friends’ substance use (smoking, drinking and using marijuana) and parenting patterns of actions on 2453 6th to 9th grades students. The results showed adolescents’ and friends’ substance uses are reciprocally predictable. Parenting patterns of actions turned negative with increased number of substance using friends. Morton (2007) inferred that adolescents’ selection and socialization tendencies are an important part of parenting practice to provide substance use protection.
The sociocultural considerations
Coleman (1980) suggested that drug-taking behavior is a function of certain variables that emerge from the psychosocial environment of the family. Family theories don not focus on individual dynamics as the source of one’s need for drugs. Instead, they focus on the family links, interactions, and functioning patterns as principal factors for compulsive drug abuse. As a subset of psychosocial theory, family systems theory explains how the family through defective behaviors encourages, reinforces, and helps drug-seeking behavior.
Johnson (1980) suggested a theory of drug subcultures to adolescents’ substance use and abuse. The concept of subculture is not the same as a sub society or the social build up. It does not express a statistical collective (as adolescents aged 12 to 18); and it is not uniform, inert, or closed. Subcultures come about from, preserved by, and change through a complicated progression of interaction including many individuals and groups whether directly or indirectly connected.
Stanton (1980) believed that a family theory of drug abuse explains many behavioral traits of drug abusers that lack explanation by other theories. These traits are the recurring, repeated nature of addiction with associated frequent treatment dropout rates. The family hypothesis looks at changes of patterns of drug use and abuse occurred during a given period, it also explains interpersonal and background variables of drug abuse.
Social learning or modeling experiences, especially negative ones, are causal links to adolescent substance use. Within this construct are the influences of modeled behaviors, expectations concerning the role of alcohol use and their experiences surrounding substance use. Among high risk children several consistent social maladaptive behaviors are implicated. Low parental concern about alcohol use, low parental concern about adolescent alcohol use, and unawareness of the negative outcomes are of significance (Scheier, Botvin and Baker 1997). Mimicking displayed parent’s behaviors, siblings, extended family members, media images, and friends, that suggests that substance use as suitable means of coping with the problems of life. Alternatively, substance use modeling suggests the avenue to becoming admired, attractive, an adult, stylish, or hardy. All the previous demonstrations of actions influences may lead to developing a maladaptive adolescent personal schema (Botvin and Botvin, 1992).
The biological approach suggests a genetically influenced tendency to alcoholism exists in some individuals, especially the offspring of alcoholics. Assuming this theory is correct; alcohol related behaviors should present genetic influence as well. Later alcohol related behaviors become encouraged by the individual’s surrounding social and cultural norms. The surrounding social and cultural norms are those influences produced by the immediate family, extended family, friends, ethnic group, and the larger society (Schuckit, 1994).
In a social and cultural environment where the use of alcohol is usually an accepted delinquency mechanism it is an approved social norm. Further, it is a behavior which carries an inherent expectancy of good times, social reward, and social status. Into such a culturally approved norm, add the relentless advertising on TV aimed at the younger generation, the social roles and clear rewards modeled in various other media formats.
With the prevalence of use in adolescents’ immediate surroundings including their community, it is not surprising that adolescents engage in such illegal maladaptive substance behaviors. In contrast, in families and cultures where social use is unacceptable, and alcohol is not readily available, such as in Muslim nations or among religious ethnic communities such as Orthodox Jews and Conservative Christian groups. The incidence of adolescent use is nonexistent or minimal outside a religious context (Carson, Butcher, and Mineka 1998).
Anderson (2000) suggested a cultural identity theory for drug abuse, whose objective is to address substance abuse etiology through appreciating how the adolescent traits and societal environment affect building up drug related unique individuality and drug abuse. In this sense, the hypothesis suggests that drug use and abuse are results of seven change processes of drug related distinctiveness. These are individual lack of attention or will (called marginalization), individual self-esteem problems, and individual limits in identifying an identity. On societal level, two processes are worthy considering, society lack of attention (marginalization), and lack of recognition of what is a drug in subcultural groups. On the wider community level, the notions of popular culture, economic potential and educational facilities play an important role.
Choice among multiple theories in frontier communities
Analyzing the various psychological, psychosocial, and sociocultural hypothesis of adolescent drug use in frontier communities one has to consider features particular to these communities. Compared to urban, suburban, and rural communities, frontier population is poorer and with lower income, as all the 50 poorer US counties are frontiers. Second, the main economic activity in most of these communities is agriculture with the lowest US rate of medical insurance. The frontiers population has the highest rates of behavioral health problems in the US (Frontiers Education Center, 2003).
Another community related factor that needs further examination is the demographic and epidemiological changes that took place overtime. This created an issue of cultural diversity and influenced the social and sociocultural notions of frontier communities (Manson, and Altschul, 2004).
Bokhan and Gusamov (2006), examined adolescents’ mental and behavior disorders leading to substance use in Alaska, and inferred that tension lessening hypothesis, insubordinate personality besides absent motivations are the leading psychological consideration for substance use in that frontier community.
A review on adolescents substance abuse in Lake County, Oregon
Why a frontiers community?
American people characteristics date back to their experiences gained during the first 300 years needed to settle in the New World of vast free land and a frontier nature. The succession from a frontier to a mature civilization was not an easy march; it was the frontier experience that heightened the nationalism inner-self and the American individuality. This is simply how frontier contributed to form the American character or frontier theory as explained by Frederick Jackson Turner’s in 1893 (Billington, 1958).
Unique to the State of Oregon is the clear demographic division between the geographic regions east and west of the Oregon Cascades. Population numbers, social norms, political ideology, and lifestyle display the differences. As a result, these differences should influence many surveys of a given population in the State of Oregon. This creates a statistical bias toward reflecting the attitudes, norms and behaviors of the more populated urban areas west of the Cascades (O’ Hara, 2007).
Recognizing this inherent confounding factor influences on economy, social, and psychosocial impact. Abbott (2006) pointed to assessment of adolescents in such communities in the lights of co morbidity of substance use with other possible coexisting psychological disorders. In addition, Oregon government directed the Northwest Professional Consortium (1998) to assess the Eastern adolescent student population separately. Labeling it as Region 5 currently identified as EOHSC (Eastern Oregon Health Services Consortium) in their research outcomes. This lead Oregon Government to adjust the state general fund division to $17 US a head in Eastern Oregon compared to $2 US a head in Central Oregon (Center for Substance Abuse Treatment, 2006).
Yet within Eastern Oregon region (EOHSC), exists one of the largest, most isolated and least populated counties in Oregon, Lake County. Demographically the county is unlike many of its Eastern County neighbors because of its small population (less than 7,500), its rural isolation, conservative ideology, mostly Caucasian population (tables 2, 3) and severely depressed economy (table 4). Because of its uniqueness, and to achieve statistical accuracy, Lake County populations should be considered separately even from Region 5 (Department of Human Services-DHS, Lake County DataBook, 2002).
Adolescents substance abuse profile in Lake County
Epidemiological profiles aim to sum up the nature and extent of alcohol, tobacco, licit and illicit drug use and related results in Lake County.
The Oregon Healthy Teens survey is a try to examine the health and welfare of adolescents. Lake County school districts started to take part in the survey in 2004.
First survey (2005-2007) included 65 percent of 8th grade and 69 percent of 11th grade adolescents. Figure (3) shows the previous month (to survey date) use of licit and illicit substances in 8th grade and 11th grade adolescents (2008 Epi Reports of Oregon counties). Figures (4 and 5) show the trends of substance use in the previous month to survey date (2008 Epi Reports of Oregon counties). The survey displayed that alcohol is the most widely used substance in Oregon (DHS report (a), 2008). The review on substance use profile among Lake County adolescents will fulfill alcohol, tobacco, and illicit drugs use.
Alcohol abuse profile among Lack County Adolescents:
Based on data of the DHS (a) report (2008), 430 people in Lake County are alcohol abusers or alcohol dependent. Of them, 34 are adolescents (12 to 17 years), and 129 are 18 to 25 years old. Lake County adolescents start using alcohol before they are 13 years old. In 2006, 36% of eighth grade adolescents reported drinking alcohol in the last month and 15% reported over-drinking. About 11th grade adolescents, 56% reported drinking alcohol during the same period, 30% reported over-drinking, and further 13% reported driving after drinking alcohol. Comparing 2004 and 2006 figures, eighth grades adolescents’ alcohol use surpasses Oregon state average, while over-drinking is higher although less than state average.
For 11th grade adolescents both last month figures and over-use surpass state average although over-use in 2006 is less than 2004 (DHS report (b), 2008) (figure 6). Comparing data from 2001 to 2007 for Oregon State adolescents, alcohol use among eighth grade adolescent increased significantly. For 11th grade adolescents the rate of alcohol use is rising with young women showing higher rates than boys do (DHS report (c), 2008).
There are three factors to blame for underage alcohol use among adolescents in Lake County. First is easy to access, 51% of eighth grade adolescents and 81% of 11th grade counterparts reported it is easy to get beer or liquor. Second is, recognized risk of alcohol use, which is low among Lake County adolescents. Third is, parent’s disapproval, most adolescents report parent’s disapproval to smoking more than to alcohol use (DHS report (a), 2008).
Tobacco abuse profile among Lake County adolescents:
Figure (7) shows the prevalence of tobacco use among Lake County adolescents. Eighth grade teen shows a higher rate compared to Oregon adolescent of the same age group. For 11th grade adolescents the rate is nearly the same. Interestingly, the use of smokeless tobacco has much higher rates for both Lake County eighth and 11th grade adolescents with young women forming 2% of 11th grade adolescents using smokeless tobacco. The rate adolescents begin smoking before 13 years in Lake County is almost double that of their counterpart anywhere else in Oregon state in 2004 and 2006. Although buying cigarettes is illegal before 18 years, yet most teens report easy availability from retailers, friends, and parents.
In 2004 and 2006, cigarettes availability for Lake County adolescents is higher than that in the rest of Oregon. Perception of smoking hazards is less in Lake county eighth grade adolescents than in the rest of Oregon state counterparts while it is nearly the same for 11th grade teens. Parent disapproval to smoking is almost the same in Lake County as the rest of Oregon State (DHS (a) report, 2008).
Illicit drug use profile among Lake County Adolescents:
In Lake County, nearly 195 individuals aged 12 years or more abusing or dependent on illicit drugs, of them 35 adolescents are between 12-17 years, and 72 are between 18-25 years. Rates of marijuana use are less among eighth and 11th grades’ Lake County adolescents than the average state rate (6% and 13% for eighth and 11th grades adolescents respectively). For eighth grade adolescent, inhalant illicit drugs come in second place after marijuana, and for 11th grade adolescents prescription drugs come in second place (DHS (a) report, 2008).
Epidemiology and risk factors data about Lake County adolescents substance abuse
Based on data available in the Oregon’s YRBR (Osborn, and Draghia, 1997), the age at which an adolescent starts using a substance is a major risk factor. The Youth Risk Behavior Report (1997) shows that alcohol, tobacco, and marijuana adolescents’ use start before 13 years (29%, 21%, and 11% for alcohol, tobacco, and marijuana respectively). American Indian Oregonian youth showed the highest incidence of starting before 13 years (42%, 37%, and 25% for alcohol, tobacco, and marijuana respectively).
Based on data from data from the U.S. Census Bureau, 2000 and 2001 Supplementary Surveys, and 2002 to 2007 American Community Survey, the Annie E. Casey foundation report (2008) on Oregon youth risk factors looked at the following.
- Income (Poverty): According to poverty level, many adolescents live in families with low income rates than the average US family income rate. The report shows nearly 40% of adolescents below 18 years living in families with incomes lower than 200% of the US federal poverty limit.
- The report recognized that starting age of substance use is a risk factor and provides recent data that prevalence among Oregon youth is lower than Counterpart adolescent US average for smoking, alcohol, and illicit drugs use.
- Although the rates of adolescents neither attending schools nor working is almost the same or slightly higher than the US average in 2007, yet the report recognizes low-level education as a risk factor.
In Lake County, there are many high risk factors related to adolescent population. These high risk factors have been used to predict reliably the early onset of substance use and abuse. Among those identified easy availability of drugs and alcohol, the sensed unlikelihood of being caught by the police, expectation of a minor impact if caught, and the prevalence of improperly performing family systems come on the top of the list.
Therefore, it is not surprising that despite the recognized conservative, friendly, caring character of the Lake County population, the rates of substance use in the adolescent population are very high. The Department of Human Services-DHS (Lake County DataBook, 2002) summarized adolescent risk and protective factors as they relate to Lake County adolescents. Both groups correlate to community, family, school, and peer or individual domains (Appendix 2).
In 2000, the Oregon research Institute in Eugene conducted a survey using the combined tools of OADAP, and the YRBS. Therefore, survey results of 1998-2000 are not parallel to those of 2000-2002, however, the information found are still functional in prevention planning (Department of Human Services-DHS, Lake County DataBook, 2002).
Alcohol is the most prevalent substance used by US adolescent, and Lake County adolescents are no exception. In 2002, more than quarter (25.4%) of Lake County eighth grade adolescents used alcohol within 30 days before the survey compared to 24% of Oregon eight grade adolescents. Among Lake County eighth grade adolescents, 45.4% used tobacco within the same period compared to 44.7% of eighth grade Oregon adolescents.
About illicit drugs, 16.9% of Lake County eighth grade adolescents reported using illicit drugs within the same period compared to 18.3% of eighth grade Oregon adolescents. Among 11th graders, almost half Lake County adolescents (45.4%) reported using alcohol within 30 days before the survey compared to 44.7% of 11th grade Oregonian adolescents. About illicit drugs, 24% of 11th grade adolescent used illicit drugs within the same period compared to 26.5% of 11th grade Oregon adolescents. Interestingly, depression scale among eighth and 11th grade Lake County male teens was 17.2% compared to 18.7% of their counterpart adolescents in Oregon State. Among female eighth and 11th graders the depression scale was 36.3% compared to 35% of their adolescents counterparts in Oregon State (Department of Human Services-DHS, Lake County DataBook, 2002).
In 2004, 49% of Lake County eighth grade teens used alcohol at least once during the 30 day before the survey compared to 29% of their counterpart Oregonian adolescent. In 2006, the ratio dropped to 36% compared to 32% of Oregonian teens counterparts. For 11th grade adolescents the ratio was 54% compared to 45% Oregonian counterparts. In 2006, the ratio increased to 56% compared to 44% Oregonian counterparts.
About tobacco, 13% of eighth grade adolescents in Lake County smoked during the 3o days before the survey compared to 8% of Oregon State counterparts. In 2006, the ratio was almost the same for Lake County and Oregon eighth grade adolescents. For 11th grade adolescents, in 2004 28% reported smoking during the same period compared to 17% of their Oregonian counterparts. In 2006, the ratio dropped for 16% of 11th grade Lake County adolescents reported smoking during the same period compared to 15% of their Oregonian counterparts. In 2004, 6% of eighth grade Lake County adolescents reported smoking marijuana 1 or more time during the 30 days before the survey compared to 10% of their Oregonian counterparts. In 2006, the ration remained the same for both categories.
For 11th graders, in 2004 20% reported the same frequency of marijuana smoking during the same period; in 2006 13% reported smoking marijuana during the same period compared to 19% of their Oregonian counterparts (DHS (a) report, 2008).
Some of the above figures show improvement as alcohol drinking among eighth and 11th graders (as shown in figure 6). However, whether these changes are significant or not remains a query. In 2007, the Office of Applied Studies, Substance Abuse and Mental Services Administration, US Department of Health and Human Services conducted an analysis to examine changes in prevalence rates of drug use. The report examined data of 2002-2003 and 2004-2005 surveys across the US.
The report used the statistical p value to examine the null hypothesis. About Oregon State, alcohol use, tobacco, and illicit drug use reported in the last month, by age group did not show any statistically significant difference, as p value was always more than 0.05. The overall rate of awareness of the risk of marijuana smoking was significantly different because of different perception of the older age group (26 years and older). This was not reflected in younger adolescent age groups. Alcohol use and ping alcohol use did not show any statistically significant differences in all age groups as reported in last month before the surveys. Tobacco use did not show any statistically significant change (Office of Applied Studies, 2007).
Apart from numbers and figures, a real assessment of changes of epidemiological patterns should include the outcomes of prevention and treatment programs. Abstinence, education drop out, rate of car accidents because of substance abuse, less arrests related to substance use. In addition, improved school behavior and academic performance are among the outcome parameters to be included. Thus noting outcome measures is an important part of understanding the numbers (Governor’s Council on alcohol and drug abuse programs, 2007).
Prevention and interventions adolescent substance use programs: strategies and approaches
The terms intervention, prevention and treatment are often used interchangeably, despite similarities in strategies and approaches, yet, there are differences in concepts and methods. Intervention refers to a range of actions aiming to reduce or improve a specific problem behavior as substance use. These actions vary in invasiveness from repeated short conversations between an adolescent and a concerned related person (parent, teacher, or a physician). More formal actions include early intervention programs having the objective of intervening before substance use develops to more problematic behavior (abuse, dependence or addiction).
They also include intensive treatment programs targeted to stop current substance use and maintain self-restraint. Prevention programs aim to stop substance use at the onset (initiation), thus, contextually; prevention is one form of intervention (Winters, 1999).
In specific terms, intervention aims to identify current or potential problems of substance use then to motivate those at high risk to change their behavior problem. Treatment aims to provide specific interventions, which address specific needs of adolescents showing problems associated with substance use (Henry-Edwards and others 2005).
Prevention is an active process centered on generating conditions that promote and support well-being. It uses evidence-based approaches, skills, and outlined strategies to reduce risk factors, in simple terms it means to prevent conditions leading to substance use from occurring or influencing adolescents (Carboni, 2007). Prevention can take many forms, universal prevention designed to get to an entire population (adolescents) with neither consideration nor prior assessment to individual risk factors. Substance abuse educational program targeting all school children in a district is an example to universal prevention programs.
Selective prevention targets a subpopulation group known to be at higher or have specific risk factors of substance use, skills training prevention program is an example to this category. Indicated prevention programs are directed to individuals showing early signs of early substance use but did not reach the stage of clinical diagnosis. Such programs include some intervention concepts as changing a problem behavior associated with substance use (Carboni 2007).
Toumbourou and colleagues (2007) performed a systematic literature review on intervention prevention strategies aiming to reduce the harm produced by substance use. The general concept of intervention prevention strategies is to reduce substance demand and supply to adolescents.
Intervention strategies and approaches
There are three basic intervention strategies; regulatory, aiming at supply reduction, it uses low enforcement, and policing to reduce and control substance supply to adolescents. Developmental intervention strategies aim at improving the surrounding environment to achieve healthy adolescent development. Early screening and brief intervention strategy targeting high risk adolescent substance users in the form of brief interventions motivating them to stop substance use (Toumbourou and other 2007).
The Substance Abuse and Mental Health Administration identified three intervention approaches for adolescent substance use and abuse (SAMHA, 2002). Brief interventions centered on addressing and developing motivation to change problem behavior and provide skills to meet these aims. Two techniques are commonly in use; first is cognitive behavioral therapy based on social learning theory, and second is motivational interviewing. Family-based therapies with multidimensional family therapy, brief strategic family therapy and multisystem therapy being the most researched three techniques. The third approach is community-based interventions, which provide mental health services within the normal environment of adolescents (school or neighborhood settings). Examples to this intervention approach are adolescents’ community reinforcement approach, and student assistance program (SAMHA 2002).
Prevention strategies and approaches
The fundamental strategy of adolescent substance use prevention programs is to manage driving risk and protective factors whether modifiable or not aiming to change one or more of these factors. The factor (s) a prevention program aims to change is the program content (Hansen and colleagues, 2007).
Effective prevention approaches of adolescents substance use should aim at adolescents, their families, neighborhood, and schools and incorporate strategies targeting these influences. First approach is to improve adolescents’ social and critical thinking skills, second is encouraging safe and supervised recreational, enrichment, and leisure activities especially for adolescents at risk. Third is early identification and referral of adolescents at high risk, which is primarily an activity of teachers, school nurses or attendants. In the school or classroom domain, the principal prevention approaches are school community contribution to the design and delivery of a prevention program.
There should clear school policies deterring substance abuse, and school communication campaigns to support behavior norms about substance use. Finally, improvement of school management techniques and instruction methods to promote student engagement in the learning process and improve their academic performance is a fruitful prevention approach (Dash and others, 2003).
In 2007, Hansen and colleagues examined substance use prevention programs available on the national registry of effective programs from 2003. They identified a variety of content elements with no content field included in all programs, and that most programs include different approaches in a combined mixture. Based on this finding, they suggested that most programs are not theory based rather they are fitting theoretical ideas of the program developer.
Therefore, program evaluation studies do not support theory or come up with acceptable theory modification. Some may suggest there is a need for rational theories to explain substance use and prevention strategy. However, the challenge is the variability of risk and etiologic factors that cannot be included comprehensively in such a theory. They inferred the real need is to cross the gap between theory and practice.
Summary of preventive approaches
Prevention of adolescent substance abuse must be multidimensional, complex, and dynamic. It must address a number of risk and protective factors, such as life skills and resistance skills, fostering healthy self-esteem, appropriate decision-making paradigms, stress management, communication skills, and assertiveness training. They are embedded in cognitive and affective schemes; yet, require a cultural approach to be influential with diverse populations. To maintain effective results, programs must be evaluated frequently and marketed successfully. Most importantly, drug-prevention programs must be accessible to high risk adolescents (Pumariega et al, 2005).
Programs that focus on one category risk factors are limited and often attract low-risk participants. This theory is supported by an evaluation of a parent-targeted, school-based adolescent drug-prevention program, which suggested that parents who participate in a drug-abuse-prevention program already have better parenting skills and relations with their children than do nonparticipants, a factor associated with a lower risk of substance abuse. More comprehensive programs include involvement at the school and community level, outreach to families for participation, peer involvement, training for adult and peer leaders, and attention to multiple risk factors associated with substance abuse, as well as supporting life skills training (Pumariega et al, 2005).
A number of such comprehensive programs have demonstrated significant effectiveness in outcome studies. The Nebraska Network of Drug-Free Youth program was designed to delay onset of substance use and to reduce or eliminate substance use among adolescents already using, by targeting seventh through twelfth grade students. Evaluation results indicated that the program helped keep drug-free students from initiating use and helped occasional users stop or reduce use, and that mixing high-risk students with low-risk students is an effective prevention strategy. However, students of both risk groups involved in the program self-selected to participate, which may be indicative of a high level of motivation to be drug free.
Another comprehensive program, Project Northland, targeting sixth, seventh and eighth grade students in 24 school districts in northeastern Minnesota, was designed to test the efficacy of a multilevel, multiyear program addressing alcohol. Overall, students from participating districts appeared to benefit positively as compared to reference districts. However, the project seems to have been more successful with students who had not used alcohol at the start of sixth grade than with those who had initiated use, suggesting that alcohol use may be very difficult to reverse even as early as the start of sixth grade (Pumariega et al, 2005).
More recently, programs have focused on young adolescents and pre-adolescents to achieve better preventive results. The Iowa Strengthening Families Program (ISFP) and the Preparing for the Drug-Free Years (PDFY) program, both of which address the transition from nonuse of substances to initiation and progression of substance abuse, demonstrated significant delays in substance abuse initiation, while the PDFY program also delayed progression of use amongst those who initiated use. The Adolescent Transitions Program is a multilevel approach to family interventions within a middle school setting based on an ecological model for social and emotional development. It includes universal, selected, and indicated strategies to serve young adolescents and their families at all risk levels.
Despite low measured levels of engagement with families using the indicated and selected interventions, they were able to achieve significant reductions in substance abuse initiation in at-risk and typical students served. Some of the program components that can be integrated into comprehensive multilevel approaches have demonstrated limited effectiveness. These include parental psycho-educational and monitoring programs and youth adult partnerships. The Adolescent Alcohol Prevention Trial, a longitudinal multisite approach combining drug and normative psycho-education and resistance skills, has also demonstrated reduction in the average levels and rates of growth for cigarette and alcohol use (Pumariega et al, 2005).
Botvin LifeSkills Training Program
The school as a site of prevention efforts
The development and testing of approaches for preventing adolescent substance abuse have largely focused on middle/junior high school students, with schools serving as the primary setting for prevention efforts. Despite their traditional educational mission, schools have been asked to assume responsibility for a variety of social and health problems. Many states mandate schools to provide their students with programs in health education and/or tobacco, alcohol, and drug education as well as teenage pregnancy and AIDS education. Although there has been considerable debate about whether schools should provide programs dealing with health and social problems, particularly at a time when there is renewed concern about academic standards, a known fact is that schools offer the most influential access to the adolescents’ population.
Moreover, many educators are gradually recognizing that problems such as drug abuse are a significant barrier to the achievement of educational objectives. The United States Department of Education, for example, has included drug-free schools as one of its goals for improving the quality of education in this country. Table (5) summarizes the different school-based approaches for adolescents’ substance abuse prevention (Botvin and Griffin, 2005).
Resistance skills training
There are several variations on the school prevention model. A distinctive feature of these prevention models is that they place more importance on teaching students identifiable skills to resist peer and media pressures for substance use in an effective manner. Resistance skills training methods teach students how to realize situations when they will have a high possibility of experiencing peer pressure to substance use so that they may avoid such high-risk situations.
This includes teaching students what to say (the specific content of a refusal message), and how to deliver it in the most effective way possible. Another distinctive feature of these programs is using peer leaders as program providers, or as an aid to an adult provider. Almost all the studies testing social resistance skills training approaches included the role of peer leaders. The peer leaders used in these interventions are typically older students (e.g., tenth graders might serve as peer leaders for seventh graders) but sometimes peer leaders of the same age as participants may be used. The rationale for using peer leaders is that peers generally have higher credibility with adolescents than do adults in regard to decisions about risky behavior.
Research evidence supports the use of peer leaders for resistance training skills prevention strategy. Further, peer-led programs were found to be more effective than adult-led programs; however, some studies found greater effects for adult-led programs. Overall, peer leaders may be most effective when they support adult program providers especially if given specific and well-defined roles (Botvin and Griffin, 2005).
Interactive versus non-interactive prevention programs
There are two principal approaches to deal with adolescent substance use, the interactive and non interactive. The interactive approach centers mainly on interpersonal interactions. The underlying belief is peer influence is one of the most powerful causal factors in developing illegal substance use. This approach postulates that acquisition and practice of interpersonal skills, the incorporation of appropriate intrapersonal beliefs and processes.
Conjunction of developed skills with increased substance knowledge; makes adolescents develop a strong anti-drug value system. They will also acquire a more positive personal schema and the appropriate skills necessary to resist influences to engage in such maladaptive behaviors. The Interactive approach is characterized by small group participatory interactions between adolescent peers rather than the didactic or lecture format evidenced in Non-Interactive programs. The instructor in the Interactive program format serves as an initiator, informer, facilitator, and supporter in the implementation of new skills by the students. In small groups, the students discuss and hopefully acquire the newly revealed skills or understandings through applications and practice in simulated real life situations (Tobler 1986).
The foundations of Botvin lifeskills training (LST) program efficacy
(National Health Promotion Associates, Inc. 2002)
- Botvin LST program is evidence based, as 25 years of research and evaluation provide evidence base support to the program.
- The program adopts a cognitive behavioral approach to develop adolescents’ skills on what they know (cognition), and what they are up to (behavior). In this way as adolescents take part in the program, a change to their health risk behavior crops up.
- The reasons of why youth become involved in health risk behavior are many and interconnecting. The LST program works on developing three cognitive behavioral skills realms.
- Repeating and supporting skills is an important technique to attain a lifelong learning experience. Therefore, the program recognizes supplementary booster teaching meeting to increase its efficacy.
- For learned skills to be a part of the individual’s behavior and become useful, instructive and informative (didactic) approaches are not enough. Practicing these learned skills is the key to success. Therefore, LST program recognizes interactive teaching methods as facilitation, coaching, and feedback to crop up at effectively lifelong practiced prevention skills.
- Information is important in any prevention program; however, this is true if the learner picks up information that matter stresses it importance. Extra unneeded information may arouse curiosity to try; thus, LST program identifies the principle of less (selected) is more.
Botvin Lifeskills Training theoretical backgrounds
The theory behind lifeskills training is complex and interacting. LST roots in children and adolescents development theories, learning, and behavior theories, which all take part in the development of LST. Each theory provides part of the basis explaining skills development, and a different viewpoint to why these skills are important. Cognitive theories centered on gaining skills view this objective an aim by itself, since developing the capability in problem solving, intercommunication are important for healthy adolescent development. On the other hand, theories centered on behavioral outcomes, view skills development as a means to progress an adolescent to the behavioral, cultural, and social expectations.
Lifeskills training has the advantage of making adolescents take part in solving their own problems, and sharing in the process of building up the social norms. From this brief theoretical base, there are three key elements of LST (figure 8). The role of program planners and executives is to configure the teaching logic and strategies needed to develop skills; this is why training on their part is important (Mangrulkar and colleagues, 2001).
Botvin Lifeskills Training Program
Botvin LifeSkills Training (LST) program is a school based training program aiming to prevent substance abuse and violence. Its target adolescents are those in upper elementary, middle, and high schools. It is fulfilled in one year, however, a two years booster is recommended. LST program has three components that cover the domains necessary to build up skills needed for prevention of substance abuse, mainly resisting friends’ and colleagues’ persuasions and pressures (peer). Besides skills needed to avoid or correct high risk behaviors through an interactive approach. The program’s components are building up drug resistance skill making adolescent identify and confront ideas promoted by friends and media about alcohol, tobacco, and other drugs (ATOD). Second is building personal self management skills in a positive way that is to set aims and maintain their path of progress, and improving decision making by learning how to analyze a problematic situation, and considering the alternatives.
Finally, is teaching students general social skills necessary to communicate with others, and to think of healthier choices, in brief how to meet social ideals and how to mix socially with the community. The program requirements are 30 sessions over three years, the first year includes 15 classes, the second year includes 10 and the third year includes five classes, each class is about 45 minutes. On course program assessment is by measuring the outcomes through pre and post questionnaires, fidelity check lists (assess program implementation by teachers), and classroom evaluation following each lesson (National Center for Mental Health Promotion and Youth Violence Prevention, 2007).
The program design is suitable to all students irrespective of previous substance use and utilizes various information delivery techniques. Teaching skills is by either instruction or demonstration; skills analyzed to components and delivered through video sessions, an instructor, or a peer-leader. Students are encouraged to practice the skills learned and provide their feedback to help improving skills. The program can be delivered by health professional for purposes as sex education, and AIDS/HIV prevention. Finally, the LST program displays a preference for violence prevention (National Health Promotion Associates, Inc. 2002).
There are many promising and seemingly effective substance-abuse prevention programs; however, evaluation research difficulties are many. These difficulties include inability to generalize the findings, different programs approaches, different target populations, and different outcome measures. Meta-analysis is a quantitative statistical procedure that analyzes findings of many studies, thus, overcoming the problems of small samples and varied results and programs.
Meta-analysis provides answers to the critical questions in planning program prevention: What works, and How does it work? Nancy Tobler conducted three meta-analysis studies to evaluate the efficacy of interactive versus interactive approaches in drug abuse prevention. Tobler’s selection criteria were all studies included used quantitative measures to express the results; all studies were on sixth to 12th grade adolescents, and a matching control group. All studies stated a principal prevention aim (Tobler and Stratton, 1997).
The first Meta analysis study (Tobler, 1986) spotlighted the content of the programs examined. It included 98 studies covering 143 prevention programs strategies. Based on their contents; the programs were categorized into five categories, knowledge only; where the teacher presents the hazardous effects of drug use. Affective only programs relating to an external expression of emotion associated with an idea or action (as self-respect, societal values), third, is combined knowledge, and affective (these type are non interactive). Fourth, are peer programs that encourage colleagues and friends to reject drug use, support developing decision making and communication skills.
Fifth are alternatives that include community service, work or job skills, building expert skills, providing outdoor experiences, and support groups. The last two categories adopt interactive strategies, result showed programs adopting any or a combination of the non interactive policies are nearly ineffective. Programs adopting interactive strategies are effective in terms of drug use directly or indirectly by measuring drug use correlates as increasing skills, and favorable behavior changes.
The second Meta analysis study (Tobler, 1993), Tobler examined 595 studies including 120 programs and indicator for success included only self reported drug use results. In this study, interactive strategies were characteristically successful. Tobler inferred interactive prevention programs produce clinical and statistical success rates far more superior to non interactive programs. Interactive success rates were equal for both licit and illicit substances, and community spread interactive programs are even more successful. Finally, it was clear to the author that the program process is pompous to the program content, which explains why interactive programs are more successful.
The third Tobler’s Meta analysis study supported the results of the previous two, besides showing the smaller the program target population, the better the results (Black, Tobler, and Sciacca, 1998). This probably makes interactive programs valuable in preventing substance abuse in frontiers communities as Lake County.
Roona and others (2001) in their Meta analysis study built on earlier studies by Tobler confirmed that lifeskills prevention programs are more effective than social influences programs. However, their results suggested that lifeskills are more effective among preliminary and high schools adolescents but not among middle school teens.
In 2005, the Federal Office of Justice awarded Oregon State one of three unrestricted grants to center adolescent alcohol use prevention efforts on EUDL. The Enforcing Underage Drinking Laws program (EUDL) applies now in Lake County, Wallowa County, and Newport City. A federal contractor and the Pacific Institute for Research and Evaluation provide training and technical help to community alliances addressing the problem of youth underage alcohol use and youth access to alcohol (Department of Human Services 2007).
Since prevention programs need considerable effort and resources to achieve success, most if not all these programs have a political module for sustaining and support. Occasionally, the scientific evidence may be undermined, if the program planners cannot communicate the program basis or get enough support, they cannot implement the program and will get a limited impact (Gilchrist, U.S. Department of Education, n.d.).
Based on research on human development theories, Mangrulkar and colleagues (2001) categorized key life skills into three groupings. First are social skills, which include communication, negotiation, assertiveness, interpersonal, and cooperation skills. Emotional coping skills include managing stress and feeling (including anger), self-management and self-monitoring skills. Cognitive skills include decision making, problem solving skills, which are represented in determining alternative solutions, analyzing external influences (as peers and media), and understanding the consequences of an action. Mangrulkar and colleagues (2001) inferred these skills are not static and made use of separately; however, they should be put to practice together as they complementary, integrative and enforce each other.
Theories of adolescent development, learning and behavior contribute to the development of life skills approach and form its theoretical background. Mangrulkar and colleagues (2001) suggested that each theory provides a part of the foundation of life skills and no single theory can justify skills development nor can it provide a perspective on why these skills are imperative. The table presented in appendix (1) summarizes the inference of each theory on developing life skills (Mangrulkar and others 2001). Thus, the theoretical core of life skills approach is a way for adolescents to contribute in constructing norms by teaching them how to think instead of what to think, and providing them with the needed tools (Mangrulkar and others 2001).
Summary
Life skills program providers and settings
The challenging nature of methods used to apply life skill training needs professional and personal skills which may be present in program providers or need training to develop. Program providers may be social workers, teachers, parents, or health care providers. Peer leaders have the advantage of not having the authoritarian and educational approaches; however they have to be successful models to covey a credible message.
Therefore, they can be successful assistants to adult program providers (Mangrulkar and others 2001). Mangrulkar and colleagues (2001) summarized the characteristics of successful life training program providers; they have to have competence in group processes like enhancing interactions and skills to direct group members. They have to have guiding rather than dominating attitudes, respect adolescent freedom to express opinion and encourage self-esteem, and they have to be enthusiastic and supportive.
Figure (9) represents a model of skills development (adapted from Mangrulkar and others 2001).
Life skills training (LST) program description
LST program has three principle components; first is to deliver an array of general self-management skills, second is to provide adolescents with general social skills. Thus these components focus to enhance the overall adolescent competence and reduce vulnerability to social influences. Third LST component includes specific information and skills linked to drug use and support drug resistance and anti-drug attitudes. This is scheduled in 15 to 17 class periods (each is 45 minutes) targeting mainly middle school students. Ten booster sessions are given in grade eight and five more in grade nine Curriculum materials for the program are teachers’ manual and a student guide (Botvin and Griffin 2001).
Effectiveness of Botvin life skills training prevention program
Over the past 25 years, studies evaluating LST program whether small scale or large scale studies confirmed that LST results in positive outcomes about smoking, alcohol and other substances use behavioral changes especially in middle school adolescents. Studies showed that main barriers to successful implementation were lack of teachers training and program material, low funding and lack of guidance from school district personnel were major barriers (Botvin and Griffin, 2004).
Lake County Botvin Life Skills Training Program: Methods
Botvin’s life skills training program was introduced to Lake County, Oregon schools for 3-year period (1998-2000). This was work was done during the period of October 1998 to February 2000 as an informal evaluation of the Botvin prevention approach targeting 6th and 7th grade adolescents being the common time frame for substance use initiation (D’Onofri0 1997).
Participants
Before the actual implementation of the early phase of the proposed three year program, the entire 6th grade student population (102) of Lake County was given the self-report Life Skills Training Student Survey (October 1998) as a pilot study. From the 102 surveys, a random sample of 80 was drawn. The weighted number of Lakeview students compared to the small number of North County students (20 in total) was adjusted to grant including all the students of the North County based on percentages of total population represented. The survey was administered again after completing the first part of instruction, in February 2000. The sampling was again random, and the percentages were adjusted to include all the North Lake County student populations. It was noticeable that no detected significant difference between the students in the North County and the Lakeview students.
By the end of the three year program, the study included 133 adolescents of 6 th grades and 99 adolescents of 7 th grades attending three middle schools. Daly Middle School in Lakeview, Paisley Middle School grades nearly 50 miles away and North Lake middle school students 100 miles away from Lakeview. They were asked to fill self-report Life Skills Training Student Survey booklets.
Apparatuses
The Survey included 11 questions chosen from sections C and D of the survey prepared by Cornell University (appendix 3). The questions chosen intended to measure the student’s past and present licit or illicit substance use (question 1). Student perception of drug use among peers and adults (questions 2 and 3), drug refusal skills (questions 4 and 5), and decision making skills (question 6). Other measures included were media effect (questions 7, 8, and 9), question 10 intended to measure anxiety reduction mechanisms among adolescents examined, and question 11 measured communication skills (appendix 4).
Procedure
The procedure selected was the pretest-post test evaluation, in which participants answer the same questionnaire before and after LST program implementation. This should highlight the program effect on selected objectives. The survey was administered twice; in October 1998 (before program implementation) and in February 2000 (after program implementation). Administering the survey passed into stages to ensure consistency in data collection; first, each student was given an ID number, then 2 copies were made for the same student one for the pretest and the second for the pos test.
Second, survey administration and collection was done by the researcher or an assistant other than the classroom teacher to ensure honest students’ self-expression in answering the questions. No scoring to answers of the questions as reported in the Life Skills Training Questionnaire Middle School Version Instruction Guid. This was because the questions in this survey were selections from the original questionnaire dealing with substance use as a whole (tobacco, alcohol, and other drugs). Statistical analysis was done using Stats software version 2.0 from Decision Analyst, Inc.
Limitations
This study did not include a control group from any other frontier area. All efforts taken to seek cooperating of school principals of comparable student populations immediately outside Lake County such as in Modoc County, California and Harney, Oregon were unsuccessful. Thus, results of this study come only from comparing the self-reported data collected before and after the instruction period in the same population of students.
Second is the inconsistency in the total numbers of participants’ response for the pre test and post- test. This is partly because of demographic factors as the survey was administered twice (18 months apart), and was performed in three schools 50 to 100 miles apart. Therefore, the total number of students completed the pre and post-test was occasionally different because of mobilization or absence from school. Further, in other occasions, some students’ answers were inconsistent in an overlook on both booklets with occasionally ambiguous contradicting answers. These students’ complete survey results or responses (answers) to specific questions were not included and the students were considered no respondents either to the whole test or to a particular question.
Lake County Botvin Life Skills Training Program: Results
Results of this study show that substance use among 6th grade Lake County adolescents was 20.3% in 1998. In 2000 (post test) the rate was 10.8% in the same age group. Comparing self-reported substance use before and after applying Botvin life skills among 6th and 7th graders showed significant differences pretest with probability of 99.9%, z-value of 5.4429 and P value less than 0.01. Post test results were also similar in significance pointing to early age of initiation among Lake County adolescents.
Tables 1 to 11 (Appendix 5, survey results) show the pre and post-test responses of 6th grades and 7th grades students to the different question groups, which are graphically, represented in figures 1 to 11 (Appendix 5, survey results).
Statistical methods
Statistical analysis of research-retrieved data aims confirming the data obtained were not because of chance (testing the null hypothesis). In the context, significance tests estimate the evidence that data obtained provide an argument they are applicable to a population (Connolly and Sluckin 1971). Many researchers use t-test, and when normality fails they use Wilcoxon rank sum test. For non-parametric data, chi-square test, bootstrap, and Fischer randomization tests are in common use.
Another test of significance is the Z-test, which is a test of the null hypothesis of a sample of N number of independent observation. A researcher may compare proportions with a z-test when there are two groups to compare, the total sample size (number of observations) for each group is known, and the proportions for each group fall within a single category (Kenny, 1987).
In this work data are two groups to compare, the total sample size of each group is known, and the proportions for each group that falls within a single category is also known. Therefore, the researcher compared proportions using the z-test (Smucker and others 2007). The P value is the probability of being wrong in concluding that there is a true difference in the two groups (the probability of rejecting the null hypothesis, or Type I error). Traditionally, one can conclude there is a significant difference when P < 0.05. In this work, the researcher used z-test (difference between two independent proportions) to calculate the probability of significant difference. The researcher then estimated z-value, critical z-score is taken from z tables (appendix in many statistics textbooks), P is calculated as [1 – critical z-score] (Dekking and others, 2005).
Statistical analysis
Statistical analysis done by Stats 2.0 software of Decision Analyst Inc (2009), using the basic function Difference between two percentages. Group one was the pretest students’ results and group two comprised the posttest results, the number of respondents and percentage for each group were fed in the corresponding squares. The software calculated the probability of significant difference between the two groups, and the Z-value. The value 1-critical z-score (Z-value) was calculated and the P value retrieved from the corresponding table in the book Statistics for the Social and Behavioral Sciences by D. A. Kenny (1987).
For question 1 (self-report of substance use), the probability of pre test to post test significant change in 6th grade daily substance users was 95.8%, z-value was 2.0332, critical z-score was 0.97882. Thus, P-value equals 0.02 (< 0.05) pointing to statistically significant reduction in Lake County 6th grade adolescent daily substance users. For 7th grade adolescents, there were no statistically significant differences between pre test and post test patterns of substance use.
For question 2 and 3 (perception of substance use among peers and adults), sixth graders thought of half their peers are substance users (pre test to post test), z-value was 1.8643. P-value was 0.03 pointing to a significant change of concept of substance use among peers. For 7th graders, P-value was less than 0.01 for the same category pointing to a more significant change of concept.
Sixth graders change of concept about adult substance use showed significant changes in concepts about none of adults were substance users, half, and all adults are substance users. The probability of pre test to post test significant change ranged from 99.97% and 83.36%, z-value ranged from 3.6130 to 1.38383, and P value was below 0.05 for all observations. Seventh graders response on the same question showed no significant change of pre test and post test concepts.
Pre test and post test drug refusal skills (questions 4 and 5) for six graders showed significant change in who may say (no) (question 4) where probability was 99.8%, z-value was 3.1672 and P was <0.001. There was also a significant change about those who will not say (no) to the negative side pointing to the impulse of experimentation, where probability was 99.5% and P was <0.001. Sixth graders who confirmed saying (no) both pre and post test did not show significant difference. Response of 6th graders on what excuse to say did not show significant differences pre and post test. Response of 7th graders to question 4 showed no significant differences to drug refusal skills, as did their responses to question 5 shows.
About decision making skills, showed decision making skills improved among 6th grade adolescent where the probability of improvement was 97.75%, z-value was 2.2818 and P was <0.01. Among 7th grade adolescent, marked improvement in decision making skills was achieved where probability was 99.97%, z-value was 3.648, and P was <0.01.
Results on media influence were consistent among 6th graders about truthful advertisement messages (question 7) and there was no statistically significant pre to pos test result. For 7th graders, the change about the possibility that advertisement message may not be truthful was significant with a probability of 90.63%, z-value was 1.6761, and P was <0.05. For question 8, response to cigarettes advertisement (whether make the person any better).
A significant change of concept among 6th graders that cigarettes never makes (me) better occurred where probability was 99.9%, z-value was 5.1186, and P value was <0.01. In 7th graders however, significant changes occurred in all responses with P always <0.05. Question 9 measured responses on alcohol advertisement, did not show significant changes in all responses of 6th and 7th graders.
Question 10 measured adolescents’ response to anxiety. Results show statistically significant difference among 6th graders who would take a health attitude to decrease anxiety, where the probability was 98.25%, z-value was 2.3754, and P value was <0.05. Among 7th graders a significant change occurred among adolescents who will never go for health behavior as their numbers significantly decreased in post test results. Probability of change was 94.69%, z-value was 1.9345, and P was <0.05.
Question 11 measured communication skills, 6th graders showed significant improvement in post test response where probability was 99.9%, z-value was 5.0277, and P was <0.05. While 7th graders showed no significant changes between pre and post test responses.
Outcomes of the study
The self-reported data gathered from the students before and after the period of Life Skills Training, instruction in Lake County suggests an overall positive affect in reducing substance use by the 6th grade student population more than 7th graders. The difference between the before and after survey measures of knowledge, and various related skills, showed increased awareness of what substance use in relation to peers and adults for 6th graders but less with 7th graders.
Change in refusal skills after Botvin Life Skills training of adolescents in Lake County showed significant changes in saying (no) for six graders, yet, the impulse for experimentation was still greater. Seventh grade adolescents did not show any significant changes. Life Skills training showed significant improvement in decision making for both 6th and 7th graders of Lake County. The media influence on adolescents showed significant improvements in some areas but not all, and best results were noticed in relation to cigarettes advertisement. Adolescents’ behavior in response to anxiety was improved after life skills training for both 6th and 7th Lake County graders. However, improvement in communication skills was more significant in 6th graders than in 7th graders.
The overall analysis suggests than 6th graders are more responsive to life skills training and the need to a multifactor prevention approach considering specific risk and protective factors in Lake County. The data also suggest the potential of interactive approach in preventing substance use in young adolescents.
Discussion
Understanding Lake County Adolescents’ substance abuse
Although the use of many substances among adolescents shows some decline in recent years; yet, the pattern of use has changed; and new substances such inhalants and steroids display recent periodic increased use among adolescents. In 2004, the American Academy of Child and Adolescent Psychiatry (aacap) reviewed community studies about substance use. The review showed that alcohol abuse at all age groups In the US ranged from 0.4% to 9.6%. The (lifetime) overall rate of alcohol dependence among all age groups ranged from 0.6% to 4.3% in Oregon State. The lifetime US dominance of drug abuse or dependency varied from 3.3% in 15-year-olds to 9.8% in 17- to 19-year-old adolescents. The review data showed, the age at which trying substances begins has been gradually declining, especially for inhalants (aacap, 2004).
Wu and others (2003) reviewed incidence and prevalence studies on drug use and inferred there is no agreement about definition of lifetime term. Second is definition of the terms; initial use, first time use, and onset of experimentation is controversial. Determination of the age of use is also a subject of variability, is it the age of first trial, or the age at which the first symptom (s) appears? Third observation is, both longitudinal and cross-sectional studies have design and sampling limits, of importance is the risk and protective factors variability across time was undetermined in both studies categories. For longitudinal studies, there are some specific limits including the cost, time-consuming, and drop of individuals for follow up. Therefore, Wu and colleagues (2003) suggest that interpreting studies’ results should be enlightened by the methods used.
Why Lake County
Examining demographic data and epidemiological data of Lake County displays the following figures. Adolescents up to 17 years age represent 23.6% of Lake County population, of them 19.5% of population below 15 years. Fifty nine percent of Lake County population live at 200% or more below the federal poverty level, of them nearly 25% are in need for prevention services. Less than 2% of Lake County population is receiving treatment for alcohol and other drugs abuse, and nearly 3% receive treatment for mental health disorders other than substance use. Alcohol, tobacco, or other illicit and licit drugs use by Lake County adolescents and adults are higher in than the average of Oregon State (Department of Human Services-DHS, Lake County DataBook, 2002).
Why adolescents
An analyst should look at substances use as a mass problem among adolescent and adult populations. Adolescents represent an asymmetrical share of this problem as nearly 29% of drug users belong to the young adult and adolescent population. It is true that a minority of drug user adolescent population passes to the dependence or addiction phase; however, substance use is a leading cause to violence, fraud and other illegal activities.
Concerns about adolescents’ drug use are because of their impact on cognitive functioning, learning, mood, and concentration. The health effects of these substances shows only after chronic use, so although symptoms of ill health may not show early the expectancy of having an ill adult in the future is high. At some point in development, adolescents experience physical changes, cognitive, emotional, and social functioning developments.
Therefore; dealing with adolescents substance use needs conservative, interactive, and innovative approaches (Polich and others, 1984). An observer must recognize that risk factors for adolescents’ substance use are different from those influencing adults’ use. Also, the different standards social acceptance of adolescents’ substance use, and the variability of co morbidity with other psychological problems add to the specifics of adolescents’ substance use. These are the reasons we should prevent adolescents’ substance use before maladaptive patterns become permanent lifetime behavior (aacap, 2004).
Understanding risk factors
An outstanding feature of drug research over the last few years is the increased numbers of various models and theories to explain the problem of drug abuse. In fact, this rapid growth is a sign for the need for a single, summarized, and applicable theory that would allow interested researchers to identify the existence, multiplicity, convergence, and intricacy of the problem. Current theoretical perception of risk factors is a blend of one’s relationship to self, others, society, and nature (genetic or biological). Current theories’ components are; first, initiation, substance use starts as an outcome of involvement with drug using peers (mates).
An adolescent who is easily driven (inceptively or influenced), principally with access to drugs, living in a tolerant environment to drug use is especially prone to drug use. Second is the continuation, which is the self-craving to keep on using drugs, with unawareness or carelessness about the outcomes. Third is, transition from use to abuse that is to move from an occasional irregular user in recreational occasions to a regular frequent user. This is the real hazard and is the red line, which if crossed, the adolescent passes to addiction. Because of this, an adolescent needs to engage in prevention program to help cessation. Keeping in mind that relapses are characteristic to addiction but drug users may suffer relapses, as they may occur with preventions of problems other than drugs as obesity (Lettieri and others, 1980).
Risk and protective factors, are principal targets for preventive intervention. The strength of the relationship between exposure to risk factors and the increasing possibility of developing of various behavior problems is outstanding. However, the question is the number of risk factors present is the authoritative predictor of problem behavior or present specific risk factor (s). Therefore, concurrent measurement of a wider selection of risk and protective factors is necessary to forecast the questions of starting and continuation of adolescents’ problem behaviors. Based on research evidence reducing risk factors and supporting protective ones became the focus of many prevention programs (Arthur and others, 2002).
Prevention research still needs instruments to evaluate the broad array of risk and protective factors. Monitoring is one tool; self-reported measures are a different tool that is suitable to adolescents’ surveys. Besides being cost-effective, can measure a broader array of risk and protective factors, they can be designed to suite risk and protective factors specific of a certain geographic area. Further, analysts can use self-report tools to identify changes in risk and protective factors; thus adjust priorities. However, there is no single standard self-report survey tool either for prospective or longitudinal research (Arthur and others, 2002).
Arthur and colleagues (2002) conducted a pilot study of a survey tool designed to suite Oregon State adolescents in sixth, eighth, and 11th grades. They inferred low correlation between risk and protective factors with demographic variables. Delinquency correlates better with risk and protective factors, in the peer-individual realm, risk and protective factors displayed the highest correlation with substance use. In different domains (community, laws, and social norms) risk and protective factors displayed moderate correlation with substance use. Availability of substances displayed the highest association with substance use. Within the family realm, poor supervision and discipline, and family tolerance to problem behavior showed moderate association with substance use. Low academic achievement and low school commitment proved moderate association with substance use but were the strongest risk factors in the school realm.
Understanding prevention
A prevention program is one directed to a targeted population, but does not address different groups included. An intervention is a program directed to a population subgroup considered at higher risk (Kellam and Langevin, 2007). Thus for every prevention program, there should be a frame or a structure and a strategy. The program skeleton should deal with problems of implementation and upholding (sustainability) (Nebraska Health and Human Service System, 2004).
There are two working prevention outlines; the risk and protective factors frame, and the IOM (Institute Of Medicine) prevention classification based on traits of targeted population (Nebraska Health and Human Service System, 2004).
The principal objective of the risk and protective factor prevention frame is to recognize risk factors and finds ways to minimize risks. With this, the frame focuses on and augments the protective factors that act as barriers to engaging in problem behavior. Risk factors and protective factors exist in central areas of adolescents’ lives as family, school, peers, and the community. Therefore, such a prevention program has to cover communal and cultural, personal and person-to-person relation factors. The risk and protective factor structure includes combined society efforts at all stages of planning and implementation. Such a program works in four domains namely; community, family, school, and individual-peer domain (Nebraska Health and Human Service System, 2004).
As one approach may not work for every group of the target population, different approaches may be necessary to deal with different population groups. The IOM system identifies three different approaches to choose the approach most suitable to the target group. The universal approach, the selective approach, which targets a subgroup considered at high risk. Third is the indicated approach that aims at the subgroup showing early signs of substance use (as those trying with more than one substance) (Nebraska Health and Human Service System, 2004).
Whatever the structure chosen, the structure of a prevention program aims to suit the target population; however, it may include initiatives aiming to change environmental, communal, economic, or policy circumstances. Based on this comprehensive view, a prevention program differs from a prevention policy or a prevention practice. Strategy in its simplest definition is to recognize the consummate way to achieve the advantageous outcomes expected (Nebraska Health and Human Service System, 2004).
Comments on the study results
Donovan (2007) recognized there is little attention paid to alcohol and substance use in adolescent around 12 years old (6th graders), therefore reviewed National and state surveys for alcohol use among 6th graders. The Youth risk behavior survey in 2005 (after Donovan, 2007) reports that 33.9% of 9th grade adolescents reported drinking alcohol before they were 13 years old. Donovan (2007) noticed that survey results varied because of many factors, first is the level of substance use involvement asked about in the survey (last year, last month, a sip, daily drinking…). Survey results also vary as a function of gender, age, ethnicity, and the year in which the survey was conducted. A characteristic of Lake County, Oregon population is the age group below 17 years represents nearly 25% of the population (7500), this displays the importance the importance of targeting this population in substance use prevention programs (DHS, 2002).
In 1997-1998 and 1999-2000 school years, the school adolescent population of Lake County was surveyed for alcohol and other substances use; however 6th grade adolescents were not included. Results showed that in 1998, the prevalence of Alcohol and substance use among 8th graders was 27.1% and in 2000 the rate decreased to 18.9%. The rates were significantly different from Oregon state prevalence rates (26% and 26.4% respectively) (DHS 2002). The Department of Human Services, Oregon Government issued a report on Lake County substance use based on data from 2000 to 2006 (DHS, 2008).
The report showed that 34 adolescents (12-17 years) in Lake County are alcohol dependent or abusers. Adolescents included reported alcohol use before reaching 13 years old, 36% of 8th graders reported drinking alcohol in the past month, and 15% reported binge drinking. The rate of tobacco use in Lake County teens is almost double that of their counterparts in Oregon state (smoking, 13% compared to 9% for Oregon teen) smokeless tobacco use rate was 37% compare to 12% for Oregon teens. Results of this study, although concerned with younger age, confirm the high prevalence of substance use among Lake County adolescents.
Major risk factors in frontiers communities
Adolescents’ decision of substance use is the outcome of many risk factors including social acceptability, family influence, peer and media (use promotion) effects, and substance availability (National Center on Addiction and Substance Use at Columbia University, 2005).
Community influences
The 2003 report of the Frontiers Education Center points to the following key issues about specific risk and protective factor for substance use in frontiers’ adolescents. First, there is lack of literature researching high risk behavior in frontier adolescents. Research also overlooks specific issues of risk and protective factors to drug use in this population. The report acknowledges lack of data on frontiers adolescents, and points to the relationship between poverty and serious emotional disturbances among frontier’s adolescents which may lead to substance abuse. The report also points to the lack of trust of frontier’s adolescents in health professionals to discuss their problems and assigned this to frequent turnover of health professionals in these communities.
Frontier communities’ poverty and behavioral health (psychological comorbidity) problems reflect on the problem of substance use (Frontier Education Center, 2003).
Based on Lake County data book (DHS, 2002), more than 10% of the population needs treatment for substance use of which nearly 13% are adolescents between 10 to 17 years. Further, 8% of the population needs mental health treatment services, of which 18.8% are adolescents between 10 to 17 years. Knowing that Lake County population represents 3.2% of the Eastern Oregon Region (EOHSC) population, one can appreciate how large the Lake County figures are important.
As regard poverty, the report indicates that 59% of the County population is living below 200% Federal poverty level. Armstrong and Costello (2002) reviewed community studies of adolescents’ substance use and psychiatric comorbidity and inferred that comorbidity of substance use with depression was 23.8% with alcohol and slightly higher (24.1%) with illicit drugs. Association rates of substance use and mood disorders were similar to depression with one study reported 8.3% rate of association in Oregon adolescents. Anxiety and substance use comorbidity median rates ranged between 16.2 and 18.2%. In this study, Botvin Life Skills training was successful in modifying 6th grade adolescents response to anxiety.
Armstrong and Costello (2002) also inferred that the single most important factor in progression from use to abuse and dependence is the early age of initiation. DHS report (2008) infers that age of initiation among Lake County Adolescent is before 13 years, this is confirmed in this study because of the significant differences in self-reported substance use between 6th grade adolescents and 7th graders.
Barnes and colleagues (2007) examined adolescents’ time use in relation to problem behavior and inferred that time spent indoors caring for siblings or watching TV is a modest risk factor, also involvement in extracurricular activities is a modest protective factor. They also inferred that working teens drink heavily and lack of activities to spend time links to spending more time with peers, which is a risk factor to all behavior problems including substance use. This factor is of relevance to frontiers adolescence because of poverty and lack of facilities.
Peers and family influences
Kobus (2003) recognized the research evidence that peers’ association is an important risk factor for adolescent substance use particularly smoking. However, the mechanisms of peer influences are not investigated properly with respect to their importance in designing successful substance use prevention intervention programs. Kobus (2003) suggested that social learning, problem behavior, and social network theory provide an understanding to peers influences mechanisms (the first two theories are of importance in frontiers). The author inferred that in the same peers’ influence in promoting substance use, and providing the social example for substance use, it can be used for deterring substance use. Kobus (2003) identified that peers influence is not without opposing forces, family relationships, and media can neutralize peers effect on adolescents for substance use.
Awareness and mentoring are important preconditions to family influences on prevention of adolescents’ substance use. McGillicddy and colleagues (2007) examined and inferred about parents awareness of substance use incidence, 82% of parents accurately reported their teens are smoking, 86% accurately reported their teens are drinking alcohol, whereas only 72% reported their teens are using illicit drugs. However, about teens’ frequency of substance use, parents considerably underestimate or overestimate their teens’ frequency of substance use, and the difference was larger with younger age teens. About parental mentoring, the younger the teen the less parental mentoring, and parental mentoring is at minimum on weekends, with lesser awareness of frequency, after school hours, or if parents are stressed with own problems. McGillicddy and colleagues (2007) suggested involving parents in prevention-intervention especially in cases of uncooperative teen or absent preprogram parental report.
Avenevoli and Merikangas (2003) stated that current research on the family role in adolescents substance use focuses on genetic epidemiologic studies and familial risk factors. They reviewed the literature on the association between parents, siblings smoking and adolescents’ tobacco use. Their findings showed inconsistent association between parents smoking and adolescents’ tobacco use, however the effects of siblings (probably as peers) was greater. They suggested families’ integration in the prevention studies.
In the present study, 6th grade adolescents’ perception that less peers are smoking (after life skills training) was associated with significant reduction in their self-reported rate of substance use, confirming Kobus’s results.
Media influences
Media has an influential impact on adolescents’ health and behavior, Ellickson and others (2005) studied a sample of more than 3000 middle schools adolescents. Results showed that 90% of the sample saw beer ads in television, sports or concert events, 80% looked at magazines displaying alcohol ads. Further 13% of in depth internet viewers (more than two pages) to alcohol websites were underage. Garfield and others (2003) showed that self-reported reading of magazines with alcohol ads in public settings were more than 7 million underage adolescents. Choi and others (2002) showed that tobacco advertising was a leading cause to adolescents’ change of status from experimentation to established smoking.
Strasburger and Donnerstein (1999) stated that although television is the predominant medium; yet, radio, magazines, and movies are influential media. They stated that content analysis of prime time networks drama, showed that 70% display tobacco, alcohol, or illicit drugs use, and more than half the musical videos contained substance use. Further, they inferred that for every prevention message as just say no, teen will view 25 beer or wine ads (in average). They examined correlational studies of consumption and exposure to ads and found a positive relationship.
Wakefield and others (2003) examined how media affects cigarette smoking about advertising, promotion, antismoking messages, and product placement. They inferred that media effects are complex and multifaceted, first media not only shape but also reflect social values about smoking, and media convey smoking promotion message directly to audiences. Media as a social learning mean provide and impress adolescents with attractive social models; media promotes and influences discussions on smoking. Besides, smoking media messages influence prevention intervention efforts, and strongly oppose antismoking messages.
Sargent (2005) stated that there is weak evidence to support the movies’ influence on behaviors for which movies are rated and television and video games have a stronger influence on adolescents. Sargent (2005) explained the strong media influence in that among social influences (peers, families, and media) peer and family effects are reciprocal with teens that is they influence each other with varying degrees. However, with media the influence is only in one direction that media affect teens convey whatever message convincingly and attractively.
The media influence on adolescents’ substance use is shown in the present study as indicated by the modest change in opinion about how true media messages are and the response to smoking and alcohol message in the media.
Substance refusal and social skills
Scheier and colleagues (1999) examined assertiveness, substance refusal, and personal competence as social skills included in training prevention programs. Their findings suggested that lower refusal correlates with poor academic performance, and poor competence, on the other hand, poor refusal links to high risk taking and increased substance use. They inferred that results of social skills training programs are modest regarding developing refusal skills. Scheier and colleagues (1999) identified that during the course of adolescents’ development, there is an interaction of social instructional skills; therefore, it can be difficult to recognize the role of refusal skills separate from other essential program skills.
In the current study, although communication and decision making skills showed significant improvement after life skills training; yet, refusal skills pattern showed slight change in saying no to drugs. However, there was no change in the reason of saying no. These somewhat unclear results point to the complexity of assessing refusal skills separately in agreement with Scheier et al (1999).
Prevention program evaluation
Evaluation is the procedure of analyzing performed to know if the program outcomes are right, to understand the barriers, and recognize defects. In other words it is a process aiming to identify the efficacy of current strategy functioning (Nebraska Health and Human Service System, 2004).
There are three basic units for evaluation:
- accountability: it is the ability to display to authorities involved that a program works and uses the funds effectively to achieve the aims and outcomes wished (Chinman and other, 2004).
- Fidelity (reliability), it is the extent of applying the principal components of the prevention program (Chinman and other, 2004). Adjustment (adaptation) that is the ability to change components because of changes in strategy as the program goes on (Chinman and other, 2004).
- Results (outcome) sustainability, it is the ability to uphold outcomes into the future (Nebraska Health and Human Service System, 2004).
A functional prevention program should have a satisfactory sample size for outcome evaluation. It should also cover at least 80% of the targeted population. It should be evidence-based, and should have provided staff training adding to their experience (Nebraska Health and Human Service System, 2004).
Evaluation of Botvin’ LifeSkills Training (LST) program (1982-1997)
Interim effects on smoking
Social influence frame of LST program showed efficacy in short-term smoking prevention. Many showed a smoking reduction rate between 30% and 50% at short- term. Tobacco smoking (experimental or regular) or non-smoking use as chewing tobacco showed significant reduction in overall prevalence. Testing the improving skill approaches showed 40 to 75 % improvement in smoking rates compared to controls. These studies show that generic skills training approaches to drug abuse prevention can cut cigarette smoking from 40% to 75% (Botvin, 1996). Botvin and Eng (1982); inferred that LST program can reduce regular smoking by 56% to 66% at the end of 1-year follow up. Booster sessions increase the rate to 87% (Botvin, 1996).
Results of studies examining both social influence frame and improving skills approach for interim alcohol and marijuana prevention were similar to smoking. A closer look shows that prevention effects were stronger for cigarette smoking and marijuana use than alcohol. However, about consistency, prevention was more consistent for alcohol use (Botvin, 1996).
Long-term (enduring) effects
Results from social influence approach follow up studies vary about long-term periods of smoking reduction ranging from one to four years, one study reported long-term smoking prevention for 7 years. However, most studies inferred long-term smoking prevention for 1-2 years (Botvin, 1996). These results cast shadows of doubt that school-based social influence prevention approach is not efficient to produce enduring results. In a randomized control study by Botvin and colleagues (1995), performed on seventh grade adolescents in 56 New York State public schools, LST program reduced smoking, alcohol, and marijuana use rates by 44%. When compared to controls, prevalence rates were 66% less for individual and multiple substance use (Botvin and others, 1995).
Botvin (1996) explained the factors that affect enduring LST program efficacy. First is the duration of intervention, second is the frequency of booster sessions (wearing away of the prevention approach), third is defective fidelity, finally LST program implantation based on confusing or faulty assumptions (Botvin, 1996). Botvin (1996) suggested that LST program is applicable to all ethnic population variations because of the overlap in risk and protective factors affecting substance use in adolescents among ethnic variations. Several studies confirmed this generalizability hypothesis perhaps with some adjustment to suite cultural differences (Botvin, 1996).
Findings of studies on the seventh grade adolescents
Botvin and Eng (1982) carried out a study of the LST program on smoking among 426 seventh grade teens from two schools in suburban New York City. The students’ traits were mainly white and belong to middle class families. They excluded pretest smokers; they divided the remaining students into two groups, 120 in the treatment group and 144 forming a control group. Posttest data were collected twice, at three months and one year later after the program started. Botvin and Eng (1982) inferred the first posttest at three months showed less past month smokers compared to the control group (8% and 19% respectively). Last week smoking did not show any significant differences between the two groups. Results showed the opposite trends after one year.
Another study by Botvin, Renick, and Baker (1983) compared the relative efficacy of two different frameworks of LST in prevention of smoking initiation. Their aim was to provide an efficiency test, and to examine the efficacy of booster sessions. The sample consisted of 902 seventh graders from seven public schools in suburban New York; however the student had the same traits as in the previous study. The study showed that past month smoking is significantly less in test group than controls (7% weekly group students compared to 13% in control group). At one year follow up fewer adolescents reported last month smoking (10% to 22% in control group). The study confirmed improvement of cognitive, personal attitude and behavioral changes related to non smoking.
In another study, Botvin and others (1984a) studied alcohol use in a group of 239 seventh grade adolescents from two high schools in New York. Students included were ethnically matched. The study included 94 adolescents as the treatment group and 73 matching teen in the control group. At three months, posttest did not show any significant difference between test and control group; however, six months posttest showed less reported last month alcohol use (12% in treatment group, compared to 26% in control group). Treatment group also showed lesser frequency of alcohol use than the control group.
Botvin and others. (1984b) evaluated the effects of the LST program on smoking, drinking, and marijuana use among 1311 seventh grade students from ten junior high schools in suburban New York. The students’ traits were similar to the previous studies. The authors modified the LST to suite the school where it is carried out so, they peer-led LST in four schools, teacher-led LST in four other schools and the remaining two were control schools.
They collected posttest scores four months after the preliminary pretest; thus, they included 1185 students in the analysis. Results of this study display the role that peers play, the study compared two groups one led by peers, and the other was teacher led. Self-reported last month smoking was significantly less in peer led group (15% smoked compared to 22% of the second group). Weekly and daily smoking self-reports did not show significant differences. At four months posttest, alcohol use was also significantly reduced among peer led adolescents, and marijuana adolescents’ use followed the same pattern.
Botvin and others (1990) performed a six-year follow up (longitudinal study) of the efficacy of LST on smoking among seventh grade adolescents that included 5954 adolescents. The schools involved were 56 schools in New York State, and the program was adjusted to schools’ environments with 22 schools as controls. Posttest data were collected just after and one year after program completion (Botvin and others, 1990).
They performed a follow up study six years later included 60% (3597) of the adolescents initially at seventh grade and became 12th graders at the time follow up. They inferred no result erosion occurred after six years among both the treatment and control groups (Botvin and others, 1995a). Results of the first study (1990) showed reduced rates of monthly, weekly, and daily smoking than in controls. This study highlighted the role of peers, as the peer led booster sessions’ group showed significantly less alcohol use than teacher led or control. Marijuana use followed the same pattern. In the six years follow up study (1995a), the lower rate of smoking was not eroded, and heavy smokers rate (pack or more a day) was significantly lower than controls. The six years longitudinal (follow up) study (Botvin and others, 1995a) also showed significant difference between the treatment and control groups about alcohol use but not marijuana use.
In 1989, Botvin and others (1989a) performed another study on 608 seventh grade adolescents in urban North New Jersey. This sample was mainly African-Americans (87%) and 10% Hispanic. Five hundred and twenty teens completed the program. Results showed fewer last month smoking among the treatment group.
Botvin and others (1989b) performed another study on LST program prevention of tobacco use among 471 seventh grade adolescents in New York. Hispanic adolescents comprised 47% of the sample. A preliminary posttest collected 3.5 months displayed the need to adjust the program because of difference in teachers’ strength of program implementation. Overall smoking was less in the treatment group, and the teachers’ strength of program implementation had a marginal significance. Further insignificant differences observed between control group and low teachers’ strength group.
Another study by Botvin and colleagues (1992) tested LST program efficacy on a larger Hispanic adolescents’ sample of 3153 teens in New York City. They belonged mainly to low income families with different schools’ environments and educational cultures. Posttest data were available after four months from the onset of the program implementation. Four months posttest showed significant less self-reported last month smoking among the treatment group (5.2%) compared to 7.2% among adolescent of the control group. Results of self-reported past week or past day smoking showed insignificant differences between the two groups.
In 1994, Botvin and colleagues studied the LST program efficacy on alcohol and marijuana use among mixed African-American (48%) and Hispanic (37%) 757 seventh grade adolescent. They were all of low income backgrounds, and despite these differences. Botvin and others (1994) applied the same LST program applied on white middle class adolescents; however, the program was adjusted to become culturally centered.
In 1995, Botvin and others (1995b) performed a two-year follow up to this study that included 60% of adolescents started the study in 1994. Statistical analysis of the follow up data showed no erosion of the results of the first study. At two years, the skills training group and the culturally adjusted intervention group showed significant difference in the rate of alcohol use. Compared to the control group, results were10%, 6%, and 13 % last month self-reported alcohol use in both groups respectively. Marijuana use showed insignificant differences among the three groups (Botvin and others, 1995b).
In 1997, Botvin and others evaluated the efficacy of LST program on 833 seventh grade multisubstance user adolescents (70% Hispanic, and 26% African-Americans) in New York City. Three months after starting the program, the research team collected posttest data from 87% of contributing adolescents. Botvin and others (1997) showed that LST program resulted in significant lesser adolescent alcohol use about frequency of use; amount used, and reduced drunkenness rates among adolescents of the treatment group compared to control. The study also showed that three months posttest pointed to significant reduction in the frequency of marijuana use.
Recent evaluation studies
More recently, Botvin and colleagues (2001a) studied the efficacy of LST program in a large sample of 5222 seventh grade teens (61% African-American, 22% Hispanic). In this study two different prevention programs were implemented, LST for the treatment group followed by booster sessions at eighth grade (2144 teen in 16 schools). The control group composed of 1477 seventh grade adolescents of 13 schools received a regular prevention program. In the treatment group posttest data were collected at 3 months and one year intervals. For the treatment group no erosion of program outcomes occurred because of the booster sessions.
At three months posttest there were insignificant differences between treatment and control group about frequency and amount of alcohol use. At one year follow up, both frequency and amount of tobacco used were less in treatment group which points to how important booster sessions are. About alcohol use, irrespective of school environment differences, the frequency of drunkenness not alcohol use was less in the treatment group. At one year follow up, adolescents’ self-reports displayed less frequent alcohol use, lesser amounts used and less frequency of drunkenness. Normalizing the results about the schools’ differences, there were no significant differences about marijuana use in the treatment and control groups at three months and one year posttests.
Botvin and colleagues (2001b) followed up the same adolescents’ sample in their eighth and ninth grades. Fifty eight percent of the starting sample continued both the one and the two years follow up assessment. At one year follow up only binge alcohol users were significantly less, and at two years follow up, the binge users’ rate remained low.
Spoth and others (2002) tested the efficacy of LST on 1664 seventh grade teens from 36 rural schools in the Midwest. However, the research team applied Strengthening Families program (SFP) in conjunction to LST. After one year the research team collected posttest data from 83% of the student sample included. After one year of program implementation, Spoth and colleagues found no significant difference between treatment and control groups concerning initiation of smoking. About alcohol use, combined LST and Strengthening Family Program resulted in significant lower rates of alcohol use in the treatment group. While the LST only adolescent less significant program outcome. About marijuana, the rate of new users was significantly lower in the combined programs treatment groups.
Griffin (2003) applied Botvin methods used in the (2001a) study to examine the efficacy of Botvin’ LST program in a group of identified high social risk adolescent. The sample consisted of 15% of Botvin’s 5222 sample (2001a). At one year follow up, Griffin and colleagues reported significantly reduced rates of alcohol use but not marijuana among the treatment group.
As stated in an earlier study by Tobler (1986), Botvin Life Skills is an interactive approach to substance use prevention, which centers on interpersonal interactions. The approach features small group participatory interactions lead by a peer. Therefore, peer training is important for adolescents’ acquisition and practice of skills developed. Of equal importance is to integrate proper beliefs and processes into the everyday adolescent activities.
Buhler and others (2007) examined 442 fifth grade adolescents involved in life skills training for substance use prevention. Their results showed students’ increased knowledge of life skills met students’ refrain from substance use, further a significant number of smoking adolescents stopped and none of the experimental smoker or non smokers turned to smoking. Buhler et al (2007) concluded that life skills training is , as research shows, the most effective single school based substance use prevention program. Botvin and others (2003) examined the effectiveness of life skills training on children and adolescents of third to 6th grades. Results showed that annual smoking prevalence rate was reduced by 61% and the same rate for alcohol use was reduced by 25%. They suggested that life skills training program is successful in substance use prevention for middle and elementary schools.
Elliot and Mihalic (2004) looked into the process of replication of a successful prevention program as the main cause of variability of results. Their argument focused on five areas where replication defects may occur, first is selection of the site where the program to be implemented. They identified five elements for site selection, a suitable site is one connected to a respected local champion, a site with influential supporting administration, a site with organizational commitment and staff stability.
Other conditions of site selection are; a site with needed resources, a site where the credibility of the chosen program is appreciated by the local community, and a site that has the potential for making the program a routine practice. The second area for problematic replication is staff (program leaders) training; they acknowledged the main obstacle in achieving this is staff turnover. Program staff should possess eligibility requirements, and administration should be encouraged to attend the training to ensure a cooperative path between administrators and program staff, which is on factor ensuring sustainability. Third is technical assistance to program staff by the program developers to overcome application difficulties. Of importance is their observation that technical assistance from program providers tend to decline over time even during the initial two years supported program implementation.
In addition, technical assistance support teams are occasionally hard to find which leads to either delay or defect in program replication. Fourth is program sustainability, which depends on affording all previous condition in addition to financial funding after the period granted (usually two years). Finally is the issue of program fidelity that is applying the core components of the program without modifications or what is known as fidelity adaptation balance.
Community tailored versus National prevention-intervention programs
Adopting national substance use prevention intervention programs achieves three important objectives; first as the problem is a nationwide problem, there is a need for a national strategy to face. Second is the development of a national strategic prevention network and third is to ensure scientific-based prevention strategy (science to service) (Curie, 2005).
Currently there are two working prevention schemes, the risk and protective factors frame whose objective is to strengthen protective factors and minimize risk factors. The second is the IOM (Institute of Mental Health) frame, which recognizes there are three approach to choose from, the universal, the selective (for a particular subgroup at high risk), and the indicated approaches (targeting a subgroup with early signs of substance use).
Whatever frame chosen it remains essential that a program should suit the targeted population, and includes initiatives to change socioeconomic, environmental, and political circumstances (Nebraska Health and Human Service System, 2004). Adolescents of Lake County, as a frontier, have specific risk factors, besides poverty, comorbidity with psychological problems, the early age of initiation of substance use, which represent a challenge to prevention programs implementation.
Elliot and Mihalic (2004) consider no contradiction between fidelity and modifying a program to suite local environment, since fidelity is applying the core components not the whole program as it is. Further, they identified that local environment is ever changing, which calls for continuous monitoring of program implementation, and program modification does not mean controlling the program elements. Finally, they acknowledged that implementing fidelity in prevention programs modified to suite specific communities is a higher level of implementation that needs special training and knowledge.
Botvin and colleagues (1998) examined the effectiveness of school-based prevention approaches and stated, since affective education is superior to information dissemination, psychological factors as etiological elements must be recognized and accounted for in program implementation. They realized that affective education is an essential component in training programs, besides, the social influence approach has three major components, psychological inoculation, resistance skills, and correcting normative expectations. They inferred a comprehensive successful prevention should include all these components (multi-component strategy).
Botvin and Griffin (2001) stated although the generalizability of life skills training is shown in the literature; yet, they realized that strongest prevention programs stem from approaches specifically designed to suite a particular targeted population. They clarified how to modify life skills training using the core or generic life skills of the program and skills specific to community where the program is applied. They emphasized that such a combination would results in better prevention results.
Sloboda and colleagues (2008) recognize the challenges in applying successful prevention programs to a particular community are to determine the extent of fidelity, examining the content and how well it covers the local community. They also identified the lack of standardized definitions, and measurements of contents (content analysis methodologies).
One last comment
The previous discussion might appear confusing about the usefulness of Life skills as a prevention approach, however successful implementation of the program needs providing apt information about substance use. Implementation of Life skills needs sociocultural community readiness that is the extent of how a community is prepared to plan for, take action, and contribute to solve a problem. Readiness is an essential association to strategy selection, since different prevention strategies are suitable for various levels of community readiness. The principal questions about Life Skills are how to measure its outcome, and of equal importance, what are the outcomes sought.
There may different viewpoints about the satisfactory outcomes, some think they are to stop substance use, and some think it is what to drink rather than how to drink. An inherent problem not only for Life Skills is adjustment to psychosocial and person-to person variables (WHO, 2003). Another factor that might be responsible for the variability of results is the diversity of program providers, as some are colleges’ students; some are members of research teams, or schoolteachers. It is clear from the previous review that peer leadership is important to achieve satisfactory outcomes, so selection and training of program providers is an essential part of a successful LifeSkills Implementation (Botvin, 1996).
A successful Life Skills or any other substance abuse prevention program needs long-term instrument, research, and funds, besides active student involvement, user-friendly materials and peer leadership modules. It remains that LifeSkills contributes to behavior development building up a positive behavior to adjust effectively to the stress of daily life. It can be useful in prevention of other youth problems as violence, and self-destructive behavior. Sex education based on Life skills may contribute to prevent AIDS/HIV spread (WHO, 2003).
Early adolescence (6th to 8th graders) represent a crucial time for adolescents to engage with, motivate, and guide young teens. During early adolescence, teen often experiment new behaviors and develop attitudes. Without guidance and support, these experimental behaviors may lead to life changing outcomes. Sixth to eighth graders are particularly potentially prone to dangerous peer influences. In addition, because of developmental concerns; they are vulnerable to health effects of substance abuse (Spencer and others, 2006).
The key to a successful prevention program for this age group is to overlook the linear psychological health model, with risk factors at one end and outcomes at the other. Instead, a successful program should consider the social settings and life course between these two points (Spencer and others, 2006). At this age, family involvement is important; Spencer and others (2006) inferred that at this age family criticism of a behavior correlates more to stress than encouragement.
Conclusions
Alcohol, tobacco, and other substance use are key public health problems that grasped community, educational and health authorities concerns, as it starts during adolescence to produce its bad aftermath in adult life. Prevention intervention programs resulted in minimal effects on drug use patterns and prevalence over the past 20 years.
Reviewing the literature shows that multi-component programs, community based or modified to address specific risk and protective factors of targeted population result in better outcomes. Besides, evidence shows that interactive strategies are more effective than non-interactive ones. Programs addressing multiple substance use have more impact as the programs designed to address other specifics, as age, ethnicity, and other population characteristics are more favourable. Peers’ and media influences appear to be major risk factors for any targeted population.
Lake County as almost all frontier communities has certain characteristics that should be considered in implementing a prevention program. Poverty, early initiation of substance use, and comorbidity with psychological health problems are important characteristics to consider.
This study evaluated the effect of Botvin Life Skills Training implemented on 6th and 7th grade adolescents of three Lake County middle schools over two years. Results showed that self-reported drug use is similar or even higher than rates of Oregon State, changes in risk behavior or improve skills change were modest pre-test compared to post test responses. Overall analysis suggests than 6th graders are more responsive to life skills training and the need to a multifactor prevention approach considering specific risk and protective factors. The interaction and complexity of risk factors are significant explanations for these results.
The LifeSkills training program (LST) is an interactive key program for adolescent substance abuse nationwide. The program works on reducing the effects of risk factors and supporting the protective factors, more important it teaches skills connected to social resistance and augments personal resilience. The reviewed finding of LST evaluation studies (small groups, large groups), in different adolescent populations display that LST program induces consistent positive behavior outcomes on substance use.
The lack of measures to determine the extent of fidelity and content analysis are challenges to overcome. Programs planned for substance abuse prevention should maintain enough time to achieve desirable results; LST was applied for less than two years and this is, perhaps, another cause for the modest results. In addition, suitable duration of program implementation ensures better long-term results, prevents relapses, and of more importance guards against the transition from substance use to abuse and dependence. In the lights of numerous references and research on adolescent substance use, the challenge remains how to cross the gap between research and practice.
Another challenge is how to replicate and disseminate successful programs, and to appreciate that substance use prevention programs are not health care and produce its effects if applied on a wide scale. Prevention programs’ settings are in the real world where risk factors interact, change from an area to another and from time to time, coping with these variations is an important step to success. Multi-component interactive community modified prevention programs implemented in schools environment remain the gold standard of prevention.
Future research should focus on some defective realms in understanding programs designed for substance use prevention and implementation. Research should address the arbitrary instruments through which LST and other programs are efficient. The most advantageous program length to produce enduring impact, an instrument that addresses identifying the most influential risk factors is other areas of needed research. Research needs also to address the problem of transition from substance use to abuse, especially about the deciding factors, program modifications to meet this hazard. Besides, what specific interventions needed to face this problem or prevent it?
References
Abbott, P. J. (2006). Co-Morbid Alcohol/Other Drug Abuse/ Dependence and Psychiatric Disorders in Adolescent American Indian and Alaska Natives. Alcoholism Treatment Quarterly, 24 (4), 3-21.
aacap (American Academy of Child and Adolescent Psychiatry) (2004). Practice Parameters for the assessment and Treatment of Children and adolescents with Substance Use Disorders. Web.
Anderson, T. L. (2000). Sociology of Crime, Law, and Deviance (Vol. 2) (Ulmer, J. T. Editor). Albany: Jai Press.
Armstrong, T., D., and Castello, E., J. (2002). Community Studies on Adolescent Substance Use, Abuse, or Dependence and Psychiatric Comorbidity. Journal of Consulting and Clinical Psychology, 70(6), 1224-1239.
Arthur, M., W., Hawkins. J. D., Pollard, J. A., and Baglioni, A., J., JR. (2002). Measuring Risk and Protective Factors for Substance Use, Delinquency, and Other Adolescent Problem Behaviors: The Communities That Care Youth Survey. Evaluation Review, 26 (6), 575-601.
Australian Government Repatriation Medical Authority. (2008). Statement of Principles concerning drug dependence and drug abuse No. 16. Melbourne: Federal Register of Legislative Instruments.
Avenevoli, S., and Merikangas, K., R. (2003). Familial influences on adolescent smoking. Addiction, 98 (Suppl.1), 1-20.
Barnes, G., M., Hoffman, J. H., Welte, J., W. et al. (2007). Adolescents’ Time Use: Effects on Substance Use, Delinquency, and Sexual Activity. Journal of Youth and Adolescence, 36, 607-710.
Bartle, P. (2007). What is community? A sociological Perspective. Web.
Benner, D.G., and Hill, P.C. (1999). Baker Encyclopedia of Psychology and Counseling. Grand Rapids, Mi: Baker Academic.
Beman, D., S. (1995). Risk factors leading to adolescent substance abuse. Web.
Billington, R., A. (1958). How the Frontiers Shaped the American Character. American Heritage Magazine, 9 (3), Cover Story.
Black, D., R., Tobler, N., S., and Sciacca, J., P. (1998). Peer Helping/Involvement: An Efficacious Way to Meet the Challenges of Reducing Alcohol, Tobacco, and Other Drug Use Among Youth. The Peer Facilitator, 15 (4), 99-108.
Bokhan, N., A., and Gusamov, R. R. (2006). Mental and Behavioral Disorders in Substance Use among Adolescents under Conditions of the Far North. Alaska Medicine Journal, Supplement, 49 (2), 251-254.
Botvin, G., J., and Eng, A. (1982). The Efficacy of a Multicomponent Approach to the Prevention of Cigarette Smoking. Preventive Medicine, 11, 199-211.
Botvin, G., J., Renick, N., L., and Baker, E. (1983). The effects of scheduling format and Booster sessions on a broad-spectrum psychosocial smoking prevention program. Journal of Behavioral Medicine, 6, 359-379.
Botvin, G., J., Baker, E., Botvin, E., M., Filazzola, A., D., and Millman, R., B. (1984a). Prevention of Alcohol Misuse through the Development of Personal and Social Competence: A Pilot Study. Journal of Studies on Alcohol, 45 (6), 550-552.
Botvin, G., J., Baker, E., Renick, N., L., Filazzola, A., D., and Botvin, E., M. (1984b). A Cognitive-Behavioral Approach to Substance Abuse Prevention. Addictive Behaviors, 9, 137-147.
Botvin, G., J., Batson, H., W., Witts-Vitale, S., Bess, V., Baker, E., and Dusenbury, L (1989 (a)). A Psychological Approach to Smoking Prevention for Urban Black Youth. Public Health Reports, 104 (6), 573-582.
Botvin, G., J., Dusenbury, L., Baker, E., James-Ortiz, S., and Kerner, J. (1989 (b)). A Skills Training Approach to Smoking Prevention among Hispanic Youth. Journal of Behavioral Science, 12 (3), 279-296.
Botvin, G. J., Tortu, S, Baker, E., and Dusenbury, L. (1990). Preventing Adolescent Cigarette Smoking: Resistance Skills Training and Development of Life Skill. Special Services in the Schools, 6, 37-61.
Botvin, G., and Botvin, E. (1992). Adolescent Tobacco, Alcohol, and Drug Abuse: Prevention Strategies, Empirical Finding, and Assessment Issues. Developmental and Behavioral Pediatrics, 13 (4), 290-301.
Botvin, G. J., Schnike, S. P., Epstein, J., A., and Diaz, T. (1994). Effectiveness of Culturally focused and Generic Skills Training Approaches to Alcohol and Drug Abuse Prevention among Minority Youths. Psychology of Addictive Behaviors, 8, 116-127.
Botvin, G., J, Baker, E., Dusenbury, L., Botvin, E., M., and Diaz, T. (1995a). Randomized Drug Abuse Prevention Trial in a White Middle-Class Population. Journal of the American Medical Association, 273 (14), 1106-1112.
Botvin, G., J., Schinke, S., P., Epstein, J., A., Diaz, T., and Botvin, E., M. (1995b). Effectiveness of Culturally focused and Generic Skills Training Approaches to Alcohol and Drug Abuse Prevention among Minority Youths: Two-year follow-up. Psychology of Addictive Behaviors, 9 (3), 183-194.
Botvin, G. J. (1996). Preventing Drug Abuse through Schools. Intervention Programs that Work, Washington, D.C.
Botvin, G., J., and Schnike, S. (Eds) (1997). The Etiology and Prevention of Drug Abuse among Minority Youth. New York: The Haworth Press, Inc.
Botvin, G., J., Botvin, E., M., and Ruchlin, H. (1998). School-Based Approaches to Drug Abuse Prevention: Evidence for Effectiveness and Suggestions for Determining Cost-Effectiveness (NIDA Research Monograph 176) [Bukoski, W., J., and Evans, R., I. (editors)]. Cost-Benefit/Cost Effectiveness Research of Drug Abuse Prevention: Implications for Programming and Policy. National Institute of Health. Rockville.
Botvin, G., J., and Griffin, K., W. (2001). Life Skills Training Theory, Methods, and Effectiveness of a Drug Abuse Prevention Approach. In Wagner, E., F., and Waldron, H., B. (editors), Innovations in Adolescent Substance Abuse Intervention. New York: Elsevier Science.
Botvin, G., J., Griffin, K., W., Diaz, T., Williams, M. (2001a). Drug Abuse Prevention among Minority Adolescents: Posttest and One-Year Follow-up of a School-Based Preventive Intervention. Prevention Science, 2 (1), 1-13.
Botvin, G., J., Griffin, K., W., Diaz, T., Williams, M. (2001b). Preventing Binge Drinking During Early Adolescence: One- and Two-Year Follow-Up of a School-Based Preventive Intervention. Psychology of Addictive Behaviors, 15(4), 360-365.
Botvin, G., J., Griffin, K., W., Paul, E., et al (2003). Preventing Tobacco and Alcohol Use among Elementary School Students through Life Skills Training. Journal of Child & Adolescent Substance Abuse, 14(2), 1-17.
Botvin, G., J., and Griffin, K., W. (2004). Life Skills Training: Empirical Findings and Future Directions. The Journal of Primary Prevention, 25(2), 211-232.
Botvin, G., J. and Griffin, K., W., (2005). School-Based Programs. In Lowinson, J., H., Ruiz, P., Millman, R., B. and Langrod, J., G., ed. Substance Abuse: A Comprehensive Textbook. 4th edition. New York: Lippincott Williams & Wilkins, Chapter 76, P. 1227.
Brain Institute-Division of Addiction Medicine- The University of Florida. (2007). Epidemiology of Adolescent Alcohol Abuse. Miami: Authors. Evelyn, F., and McKnight, W. L.
Buhler, A., Schroder, E., and Silbereisen, R., K. (2007). The role of life skills promotion in substance abuse prevention: a mediation analysis. Health Education Research. Web.
Burrow-Sanchez, J. (2006). Understanding adolescent substance abuse: Prevalence, risk factors, and clinical implications. The Journal of Counseling and Development, 84 (3), 283-290.
Carboni, J. (2007). Substance abuse prevention methods for middle school students. Web.
Carson, R., Butcher, J., and Mineka, S. (1998). Abnormal Psychology and Modern Life: Substance-related and Other Addictive Disorders (10th Edition). New York: Addison-Wesley Educational Publishers.
Catalano, R.F., and Hawkins, J.D. (1996). The Social Development Model: A theory of antisocial behavior. In Delinquency and Crime: Current Theories. [Hawkins, J.D. (editor). Cambridge University Press. New York.
Center for Rural Health, University of North Dakota (2006). Expert Panel Report Defining the Term “Frontier Area” for Programs Implemented through the Office for the Advancement of Telehealth. Web.
Center for Substance Abuse Treatment (2006). Oregon Uniform Application FY 2007: Substance Abuse Prevention and Treatment Block Grant. Web.
Chassin, L., Tetzloff, C., and Hershey, M. (1985). Self-Image and Social-Image Factors in Adolescent Alcohol Use. J. Stud. Alcohol, 46, 39-47.
Chinman, M., Imm, P., and Wandersman, A. (for RAND Health). (2004). Getting To Outcomes 2004 Promoting Accountability Through Methods and Tools for Planning, Implementation, and Evaluation. Santa Monica.
Choi, W., S., Ahluwalia, J., S., Harris, K., J., et al (2002). Progression to established smoking: The influence of tobacco marketing. Am. J. Prev. Med., 22(4), 228-223.
Colby, J., and Witt, M (Authors): United Nation’s Children’s Fund-UNICEF. (2000). Defining Quality in Education. New York.
Coleman, S. B., National Institute on Drug Abuse. (1980). Theories on Drug Abuse: Selected Contemporary Perspectives. Rockville: Department of Health and Human Service: Alcohol, Drug Abuse, and Mental Health Administration.
Columbia, K (October 2005). Addressing generational diversity. International Journal of Newspaper and Technology. Web.
Connolly, T., G., Gerard, T., and Sulckin, W. (1971). Introduction to Statistics for the Social Sciences (Macmillan student editions). New York: Macmillan.
Cotton, N. (1979). The Familial Incidence of Alcoholism: A review. Journal of Studies on Alcoholism, 40 (1), 89-116.
Cuijpers, P. (2002). Peer-Led and Adult-Led School Drug Prevention: A Meta analytic Comparison. J. Drug Education, 32(2), 107-119.
Curie, C. (2005). Testimony on Substance Abuse Prevention and Mental Health Services Administration before Subcommittee on Criminal Justice, Drug Policy and Human Resources, United States House of Representatives. Web.
D’Onofrio, C. (1997). The Prevention of Alcohol Use by Rural Youth. In NIDA Research Monograph 168 [Robertson, E. B., Sloboda, Z., Boyd, G. M., Beatty, L., and Kozel, N., J. (editors)]. National Institute on Drug Abuse. Rockville, MD (250-346).
Dakof, G. A. (2000). Understanding Gender Differences in Adolescent Drug Abuse: Issues of Comorbidity and Family Functioning. Journal of Psychoactive Drugs, 32(1), 25-32.
Dash, K., Whitman, C., V., Harding, W., Goddard, C., et al (2003). Applying effective strategies for school violence and substance abuse prevention. Newton, Ma: Education Development Center, Inc.
Dawes, M. A., Mathias, C. W., Richard, D. M., Hill-Kapturczak, N., and Dougherty, D. M. (2008). Adolescent Suicidal Behavior and Substance Use: Developmental Mechanisms. Substance Abuse: Research and Treatment, 2, 13-28.
Dawson, D., Harford, T., & Grant, B. (1992). Family History as a Predictor of Alcohol Dependence. Alcoholism: Clinical and Experimental Research, 16 (3), 572-575.
Deas, D., and Thomas, S. (2002). Comorbid Psychiatric Factors Contributing to Adolescent Alcohol and Other Drug Use. Alcohol Research and Health, 26 (2), 116-121.
Dent, C., W., Grube, J., W., and Biglan, A. (2005). Community level alcohol availability and enforcement of possession laws as predictors of youth drinking. Preventive Medicine, 40, 355-362.
Dekking, F., M., Kraaikamp, C., Lopuhaa, H., P., and Meester, L., E. et al. (2005). A Modern Introduction to Probability and Statistics: Understanding Why and How. London: Springer-Verlag.
Department of Human Services: Office of Mental Health and Addiction Services-Oregon State Government (2002). Lake County- County DataBook. Web.
Department of Human Services (DHS) Addictions and Mental Health Division. (2007). Oregon Substance Abuse Prevention Report Fiscal. Salem: Department of Human Services: Addictions and Mental Health Division.
Department of Human Services (DHS, a): Oregon State Government. (2008). Alcohol, Illicit Drug & tobacco Consumption and Consequences in Lake County, Oregon. Salem: DHS: Addictions and Mental Health Division.
Department of Human Services (DHS, b): Oregon State Government (2008). Underage drinking in Lake County. Web.
Department of Human Services (DHS, c): Oregon State Government (2008). Underage drinking. Web.
Donovan, J., E. (2007). Really Underage Drinkers: The Epidemiology of Children’s Alcohol Use in the United States. Prev Sci, 8(3), 192-205.
Ellickson, P., L., Collins, R., L., Hambarsiimians, K., et al (2005). Does alcohol advertising promote adolescent drinking? Results from a longitudinal assessment. addiction, 100(2), 235-246.
Elliot, D., S., and Mihalic, S. (2004). Issues in disseminating and replicating effective prevention programs. Prevention Science, 5, 47-53.
Fagg, D. (2006). Adolescent Drug Use. Revolve, 13, 1-15.
Frontier Education Center. (2003). Frontier communities: Leading the Way with Innovative Approaches to Behavioral Health. Santa Fe: National Clearinghouse for Frontier Communities.
Galea, S., Nandi, A., and Vlahov, D. (2004). The Social Epidemiology of Substance Use. Epidemiologic Reviews, 26, 36-52.
Gallois, C., Ogay, T., and Giles, H. (2005). Communication theory: A look back and a look ahead [Gudykunst (Ed)]. Theorizing about intercultural communication. Sage. Thousand Oaks, CA.
Garfield, C., F., Chung, P., J., and Rathouz, P., L. (2003). Alcohol advertising in Magazines and Adolescent Readership. JAMA, 289(18), 2424-2429.
Gilchrist, L., D. (n.d.). Archived Information: Current Knowledge in Prevention of Alcohol and Other Drug Abuse. Web.
Goodwin, D. (1986). Heredity and Alcoholism. Annals of Behavioral Medicine, 8, 3-6.
Goodwin, D. (1984). Studies of Familial Alcoholism: A Review. Journal of Psychiatry, 45(12), 14-17.
Gordon, H., W., and Glantz, M., D. (1996). Individual Differences in Biobehavioral Etiology of Drug Abuse. National Institutes of Health, U.S. Department of Health and Human Services. Rockville, MD (16-48).
Governor’s Council on Alcohol and Drug Abuse Programs (2007). Effectiveness Report. Web.
Griffin, K., W., Botvin, G., J., Nicholas, T., R., and Doyle, M., M. (2003). Effectiveness of a Universal Drug Abuse Prevention Approach for Youth at High Risk for Substance Use Initiation. Preventive Medicine, 36, 1-17.
Griffin, K., W., Scheier, L., M., Botvin, G., J., and Tracy, D (2001). Protective role of personal competence skills in adolescent substance use: Psychological well-being as a mediating factor. J. Psychol Addict Behav, 15, 194-203.
Gullotta, T., P., Adams, G., R., and Ramos, J., M. (2005). Handbook of Adolescent Behavioral Problems Evidence-Base Approach to Prevention and Treatment. New York: Springer.
Hansen, W., B., Dusenbury, L., Bishop, D., and Derzon, J., H. (2007). Substance abuse prevention program content: systematizing the classification of what programs target to change. Health Education Research, 22(3), 351-360.
Hawkins, E., H., Cummins, L., H., and Marlatt, G., A. (2004). Preventing Substance Abuse in American Indian and Alaska Native Youth: Promising Strategies for Healthier Communities. Psychological Bulletin, 130(2), 304-323.
Hecht, M., L., and Krieger, J., L., R. (2006). The Principle of Cultural Grounding in School-Based Substance Abuse Prevention the Drug Resistance Strategies Project. Journal of Language and Social Psychology, 25(3), 310-319.
Henry-Edwards, S., Humeniuk, R., Ali, R., Montiero, M., and Poznyak, V. (2005). Brief Intervention for Substance Use: A Manual for Use in Primary Care. Geneva: Department of Mental Health and Substance Dependence, WHO.
Johnson, B. D., National Institute on Drug Abuse. (1980). Theories on Drug Abuse: Selected Contemporary Perspectives. Rockville: Department of Health and Human Service: Alcohol, Drug Abuse, and Mental Health Administration.
Johnston, L.D., O’Malley, P.M., & Bachman, J.G. (2003). Monitoring the Future National Results on Adolescent Drug Use: Overview of Key Findings, 2002. (NIH Publication No. 03-5374). Bethesda, MD: National Institute on Drug Abuse.
Kaminer, Y. (2005). Challenges and opportunities of group therapy for adolescent substance abuse: A critical review. Addictive behaviors, 30, 1765-1774.
Kellam, S., G., and Langevin, D., L. (2003). A Framework for Understanding “Evidence” in Prevention Research and Programs. Prevention Science, 4 (3), 137-153.
Kenny, D. A. (1987). Statistics for the Social and Behavioral Sciences. Little, Brown and Company. Canada (187).
Kim, S., Crutchfield, C., Williams, C., and Hepler, N. (1998). Toward a new paradigm in substance abuse and other problem behavior prevention for youth: Youth development and empowerment approach. Journal of Drug Education, 28(1), 1-17.
Klein, D, Shane, P., and Barry, G. (2003). Adolescent Substance Abuse Needs and Services Planning Final Report. California Association of Alcohol and Drug Program Executives, Inc. Sacramento.
Kobus, K. (2003). Peers and adolescent smoking. Addiction, 98(Suppl.1), 37-55.
Langrod, J. G., Lowinson, J. H., Millman, R. B., and Ruiz, P. (2004). Substance Abuse: A Comprehensive Textbook (Spiral Manual Series). 4th edition. Philadelphia: Lippincott Williams & Wilkins.
Lee, G., Akers, R. L., and Borg, M. J (2004). Social Learning and Structural Factors in Adolescent Substance Use. Western Criminology Review, 5 (1), 17-34.
Lettieri, D., J., Sayers, M., and Pearson, H., W. (For the National Institute on Drug Abuse). (1980). Theories on Drug Abuse Selected Contemporary Perspective. Rockville, Maryland: National Institute on Drug Abuse; Division of Research.
Lynch, W., J., Roth, M., E., and Carroll, M., E. (2002). Biological basis of sex differences in drug abuse: preclinical and clinical studies. Psychopharmacology, 164, 121-137.
Mangrulkar, L., Whitman, C., V., and Posner, M. (for the Pan American Health Organization – WHO) (2001). Life Skills Approach to Child and Adolescent Healthy Human Development. Web.
Manson, S. M, and Altschul, D. B. (2004). Cultural Diversity Series: Meeting the Mental Health Needs of American Indians and Alaska Natives. Web.
McGillicuddy, N., B., Rychtarik, R., G., Morsheimer, E., T., and Bruke-Storer, M., R. (2007). Agreement between Parent and Adolescent Reports of Adolescent Substance Use. Journal of Child & adolescent Substance Use, 16, 59-78.
Monteiro, M., & Schuckit, M. (1988). Populations at High Risk: Recent Findings. Journal of Clinical Psychiatry, 49(9), 3-7.
Morton, B-S. (2007). Social Influences on Adolescent Substance Use. Am J Health Behav., 31 (6), 672-684.
National Center for Mental Health Promotion and Youth Violence Prevention (2007). Evidence-Base Intervention Fact Sheets: Botvin Life Skills Training (LST). Web.
National Center on Addiction and Substance Abuse at Columbia University. (2005).
National survey of American attitudes on substance abuse X: teens and parents. Web.
National Health Promotion Associates, Inc. (2002). LifeSkills Planning Workbook. Web.
Nebraska Health and Human Services. (2004). SICA Guidance Document for Selecting Science-Based and Promising Substance Abuse Prevention Strategies. Lincoln: Office of Mental, Substance Abuse and Addiction Services.
NIDA (National Institute on Drug Abuse) (2000). NDA Notes (Gender Differences in Drug Abuse Risks and Treatment). Web.
O’ Hara, E. V. (2007). Oregon: From the Catholic Encyclopedia. Web.
Office of Applied Studies, Substance Abuse and Mental Health Services Administration (SAMHSA), US Department of Health and Human Services (2007). Changes in Prevalence Rates of Drug Use between 2002-2003 and 2004-2005 among States. Web.
Office of Applied Studies. (2008). Results from the 2007 National Survey on Drug Use and Health: National Findings. Rockville: Substance Abuse and Mental Health Services Administration (SAMHSA).
Office of National Drug Control Policy (a). (2002). National Drug Control Strategy. Washington, DC: The White House Office of National Drug Control Policy (ONDCP).
Office of National Drug Control Policy (b). (2002). The Evolution of Prevention Theory and Programming. Washington, DC: The White House Office of National Drug Control Policy (ONDCP).
Office of the Surgeon General. (2007). The Surgeon General’s Call to Action To Prevent Underage Drinking. Washington, DC: U.S. Department of Health and Human Services.
Oregon Office of Alcohol and Drug Abuse Programs. (1998). Pathway to a Health Future, Lake County (1998 County Substance Abuse Profile).
Osborn, A., and Draghia, D. (Editors) (1997). 1997 Oregon Youth Risk Behavior Survey. Web.
Polich, J., M., Ellicks, P., L., Reuter, P., and Kahan, J. P. (1984). Strategies for Controlling Adolescent Drug Use. Web.
Pumariega, A., J., Kilgus, M., D., and Rodriguez, L., (2005). Adolescents. In Lowinson, J., H., Ruiz, P., Millman, R., B. and Langrod, J., G., ed. Substance Abuse: A Comprehensive Textbook. 4th edition. New York: Lippincott Williams & Wilkins, Chapter 62, Pp. 1022-1038.
Resnicow, K., Soler, R., Braithwaite, R., L. et al (2000). Cultural Sensitivity in Substance Use Prevention. Journal of Community Psychology, 28(3), 271-290.
Robertson, E., B. (1997). Introduction: Interventions and Services. In NIDA Research Monograph 168 [Robertson, E. B., sloboda, Z., Boyd, G. M., Beatty, L., and Kozel, N., J. (editors)]. National Institute on Drug Abuse. Rockville, MD (246-249).
Roona, M., Streke, A, Ochshorn, P., Marshall, A., and Palmar, A. (2001). Identifying Effective School-Based Substance Abuse Prevention Interventions. InThe Robert Wood Johnson’s Foundation’s Prevention 2000: Moving Effective Prevention Programs into Practice. Princeton: The Robert Wood Johnson Foundation.
SAMHSA (Substance Abuse and Mental Health Services Administration). (2002). Report to the Congress on the Prevention and Treatment of Co-Occurring Substance Abuse Disorders and Mental Disorders (chapter 4). Washington, DC: US Department of Health and Human Services.
Sargent, J., D. (2005). Smoking in Movies: Impact on Adolescent Smoking. Adolesc Med, 16, 345-370.
Scheier, L., M., Botvin, G., J., Diaz, T., et al (1999). Social Skills, Competence, and Drug Refusal Efficacy as Predictors of Adolescent Alcohol Use. J. Drug Education, 29(3), 251-278.
Schuckit, M. (1994). A Clinical Model of Genetic Influences in Alcohol Dependence. Journal of Studies on Alcohol, 55, 5-17.
Schuckit, M., & Smith, T. (1996). An 8 year follow-up of 450 Sons of Alcoholic and Control Subjects. Archives of General Psychiatry, 53, 202-210.
Sheckter, M., E. (2000). Risk and Protective Factors for Adolescent Substance use. Unpublished doctoral dissertation, University of Saskatchewan.
Shusta, R., M., Levine, D., R., Wong, H., Z., Olson, A., T., and Harris, P., H. (2008). Multicultural Law Enforcement: Strategies for Peacekeeping in a Diverse Society. New Jersey: Pearson Prentice Hall.
Silberg, J., Rutter, M., D’Onofrio, B, and Eaves, L. (2003). Genetic and environmental risk factors in adolescent substance use. Journal of Child Psychology and Psychiatry, 44 (5), 664-676.
Sloboda, Z., Stephens, P., Pyakuryal, A., et al (2008). Implementation fidelity: the experience of the Adolescent Substance Abuse Prevention Study. Health Educ. Res. Web.
Smuker, M., Allan, J., and Carterette, B. et al. (2007). A Comparison of Statistical Significance Tests for information on Information and Knowledge Management. University of Massachusetts Amherst: Center for Intelligent Information Retrieval.
Spear, L. P. (2002). The Adolescent Brain and the College Drinker: Biological Basis of Propensity to Use and Misuse Alcohol. Journal of Studies on Alcohol, Supplement 14(14), 71-81.
Spencer, M., B., Fegley, S., and Dupree, D. (2006). Investigating and Linking Social Conditions of Minority Children and Adolescents with Emotional Well-being. Ethn Dis. 16 (Suppl 3), S3-67-S3-70.
Spooner, C. (1999). Causes and correlates of adolescent drug abuse and implications for treatment. Drug and Alcohol Review, 18, 453-475.
Spoth, R., L., Redmond, C., Trudau, L., and Shin, C. (2002). Longitudinal Substance Initiation Outcomes for a Universal Preventive Intervention Combining Family and School Programs. Psychology of Addictive Behaviors, 16 (2), 129-134.
Stanton, M. D., National Institute on Drug Abuse. (1980). Theories on Drug Abuse: Selected Contemporary Perspectives. Rockville: Department of Health and Human Service: Alcohol, Drug Abuse, and Mental Health Administration.
Strasburger, V., C., and Donnerstein, E. (1999). Children, Adolescent, and the Media: Issue and Solutions. Pediatrics, 103(1), 129-130.
Sussman, S.; Dent, C.W.; and Stacy, A.W. (2002). Project Toward No Drug Abuse: A review of the findings and future directions. American Journal of Health Behavior, 26(5), 354–365,
The Annie E. Casey Foundation (2008). Kids Count Data Center: Profiles by Geographic Area>Oregon. Web.
The National Center for Frontiers Communities. (2000). Geography of Frontier America The View at the Turn of the Century. Ojo Sarco, New Mexico: National Center for Frontier Communities.
The National Clearinghouse for Frontier Communities. (2003). Frontier Youth: Living on the Edge. Santa Fe: Frontier Education center.
Tims, F., M., and Leukefeld, C., G. (1986). Relapse and Recover in Drug Abuse. Rockville: National Institute on Drug Abuse.
Tobler, N.S. (1986). Meta-analysis of 143 adolescent drug prevention programs: Quantitative outcome results of program participants compared to a control or comparison group. Journal of Drug Issues 16, 535-567.
Tobler, N. (1993). Updated meta-analysis of adolescent drug prevention programs. In C.Montoya, C. Ringwalt, B. Ryan, & R. Zimmerman (Eds), Evaluating School-Linked Prevention Strategies: Alcohol, Tobacco, and Other Drugs. San Diego, CA: UCSD Extension, University of California, 71-86.
Tobler, N. & H. Stratton (1997). Effectiveness of school-based drug prevention programs: A meta-analysis of the research. Journal of Primary Prevention 18 (1), 71-128.
Toumbourou, J., W., Stockwell, T., Neighbors, C., et al (2007). Interventions to reduce harm associated with adolescent substance us. The Lancet, 369, 1391-1401.
United Nations Office for Drug Control and Crime Prevention. (2003). Botvin Life Skills Training Program: School-based Drug Education: a guide for practitioners and the wider community. Web.
U.S. Department of Health & Human Services. Substance Abuse & Mental Health Services Administration: Office of Applied Studies. (2008). The NSDUH Report: Underage Alcohol Use: Where Do Young People Drink? Rockville, MD: Office of Applied Studies.
Wakefield, M., Flay, B., Nichter, M., et al (2003). Role of media in influencing trajectories of youth smoking. Addiction, 98(Suppl1), 79-103.
Watkins, K., Elickson, P., Vaiana, M., and Hiromoto, S. (2006). An Update on adolescent drug use: What school counselors need to know. Professional School Counseling, 10 (2), 131-136.
Winters, K., C. (1999). Screening and Assessing Adolescents for Substance Use Disorders Treatment Improvement Protocol (TIP) Series 31. Rockville: Center For Substance Abuse Treatment: Substance Abuse and Mental Health Services Administration.
Witkiewitz, K., and Marlatt, G., A. (2004). Relapse Prevention for Alcohol and Drug Problems. American Psychiatrist, 59(4), 224-235.
Williams, P., G., Gravson, N., Holmbeck, R. (2002). Adolescent Health Psychology. Journal of Consulting and Clinical Psychology, 70(3), 828-842.
Wood, M., D., Read, J., P., Mitchell, R., E., and Brand, N., H. (2004). Do Parents Still Matter? Parent and Peer Influences on Alcohol Involvement among Recent High School Graduate. Psychology of Addictive Behaviours, 18(1), 19-30.
World Health Organization, Regional Office for the Western Pacific (WHO/WPRO). (2003). Value adolescents, invest in future: Educational package. Facilitator’s manual. Manila, Philippines.
World Health Organization (WHO). (2003). WHO Expert Committee on Drug Dependence: Thirty-third Report. WHO Technical Reports Series: 915. Geneva.
Wright, D. (2002). State Estimates of Substance Use from the 2000 National Household Survey on Drug Abuse: Volume I. Findings. Rockville: SAMHSA, Office of Applied Studies.
Wright, D., & Pemberton, M. (2004). Risk and Protective Factors for Adolescent Drug Use: Findings from the 1999 National Household Survey on Drug Abuse (DHHS Publication No. SMA 04-3874, Analytic Series A-19). Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies.
Wu, L-T., Korper, S. P., Marsden, W., E., et al (Office of Applied Studies – SAMHSA). (2003). Use of Incidence and Prevalence in the Substance Use Literature: A Review. Rockville: Substance Abuse and Mental Health Services Administration, US Department of Health and Human Services.
Tables

Table (5) Overview of major school-based prevention approaches (Botvin and Griffin, 2005).
Figures
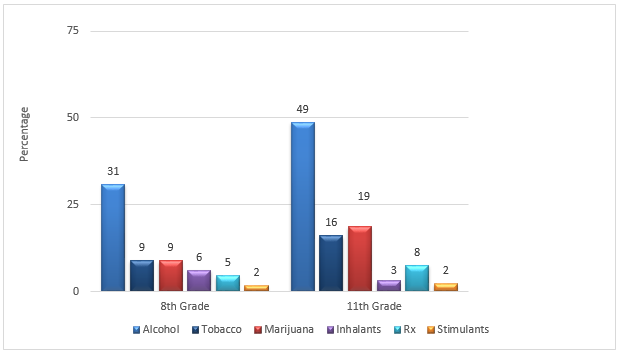
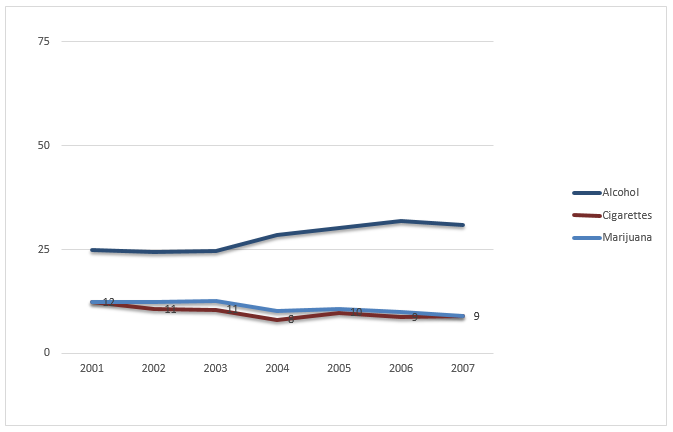
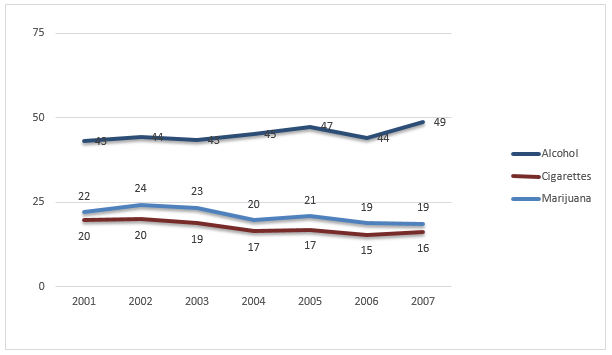
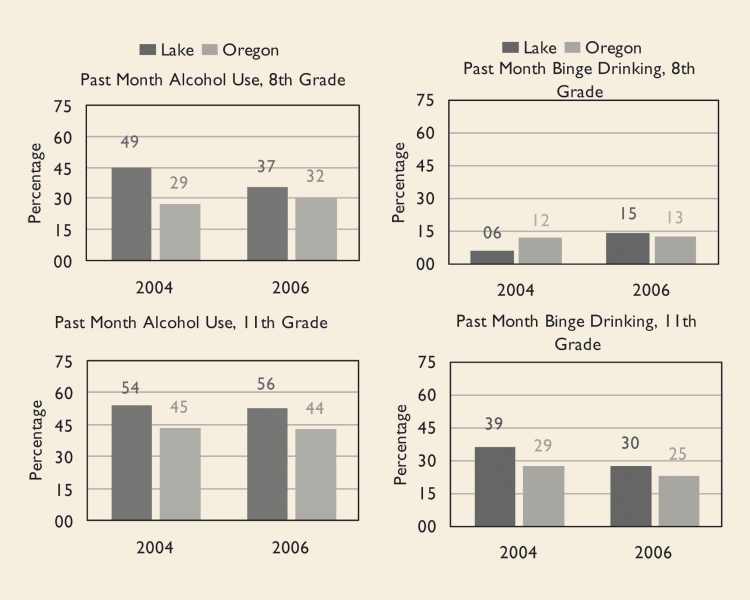
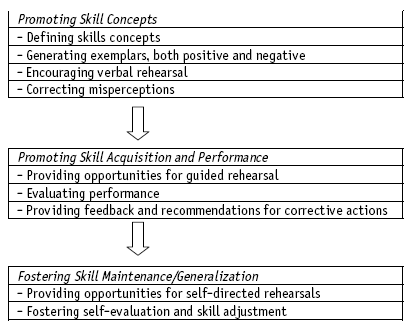
Appendix 1: Implications of theories for developing life skills
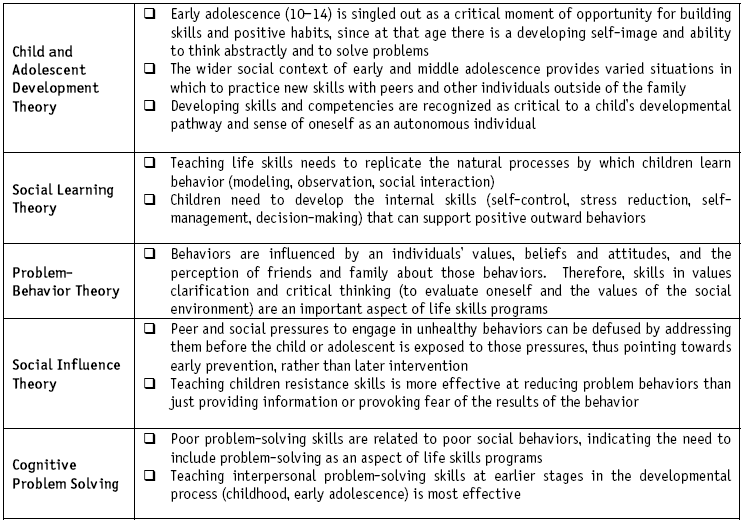
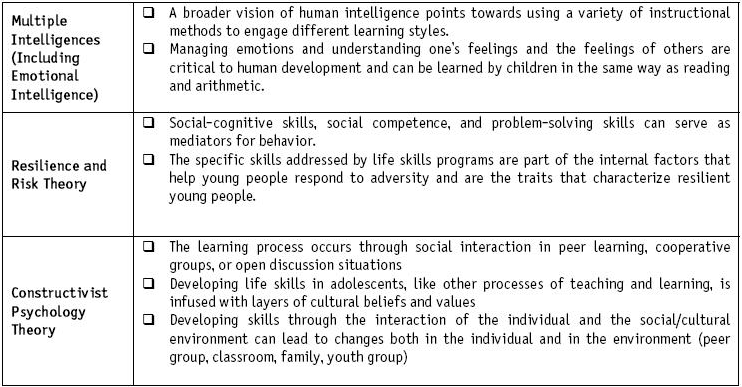
Appendix 2: Risk and Protective Factors as they apply to Lake County Adolescents
Risk factors (Continued)
Risk factors (continued)
Appendix 3: Cornell University LST Middle School Survey
Appendix 4: Questions of the study self-report on Life Skills Training Student Survey
- About how often (if ever) do you: Smoke cigarettes, drink alcohol, smoke marijuana, sniff inhalants or use other drugs?
- How many people your age do you think: Smoke cigarettes, drink alcohol, smoke marijuana, use cocaine or other hard drugs, and sniff other things to get high?
- How many adults do you think: Smoke cigarettes, drink alcohol, and smoke marijuana, use cocaine or other hard drugs?
- How likely would it be for you to say “No” when someone tries to get you to smoke cigarettes, drink alcohol, smoke marijuana, use cocaine or other hard drugs, or inhale other things to get high?
- If someone asked you to smoke, drink, use marijuana or other drugs, would you:
- Tell them no, tell them not now, I don’t want to, make up an excuse and leave?
- When I have a problem or need to make an important decision I get more information needed to make the best choice, think of ways to solve the problem, think what will happen for each choice before doing it, make the best choice and then do it.
- When I see or hear an advertisement, I think about whether what the Ad says is true, remind myself that the Ad is trying to get me to buy what they are advertising, tell myself that advertisements are not always truthful.
- When I see or hear a cigarette Ad, I tell myself that smoking cigarettes will not make my life better.
- When I see or hear an alcohol Ad, I tell myself that drinking wine, beer or liquor will not make my life better.
- When I feel anxious, I relax my muscles in my body, imagine myself in a peaceful place, tell myself to feel clam and not worry, breath slowly while I count 4 in and 4 out, practice doing whatever makes me feel nervous until I feel more confident.
- When I want people to understand me, I make sure what I say matches my tone of voice, how I stand, and the expression on y face, talk in a way that is clear and specific.
Appendix 5: Survey results
Table 1: 6th and 7th graders pre test and post test responses to question 1.
Occas = Occasional
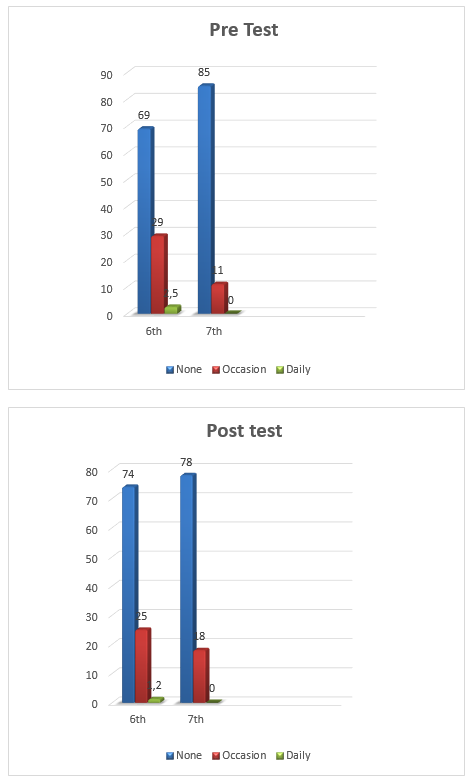
Table 2: 6th and 7th graders Pre test and post test responses to question 2.
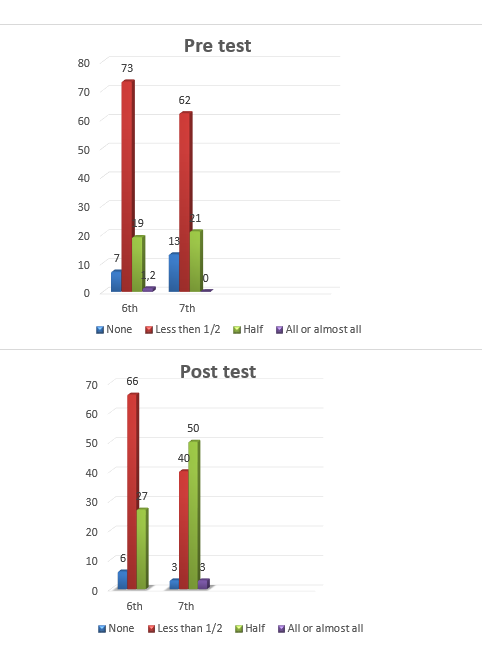
Table 3: 6th and 7th graders pre test and post test responses to question 3.
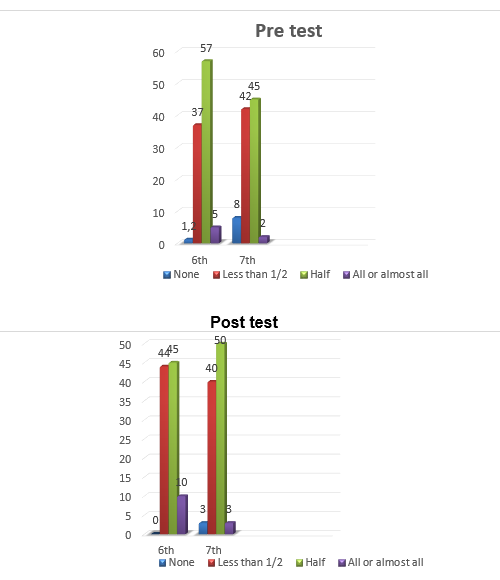
Table 4: 6th and 7th graders pre test and post test responses to question 4.
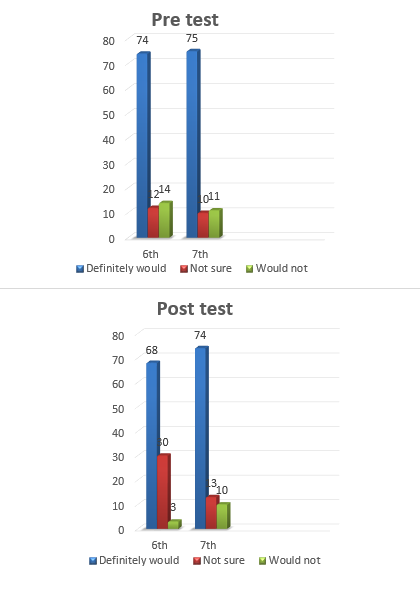
Table 5: 6th and 7th graders pre test and post test responses to question 5.
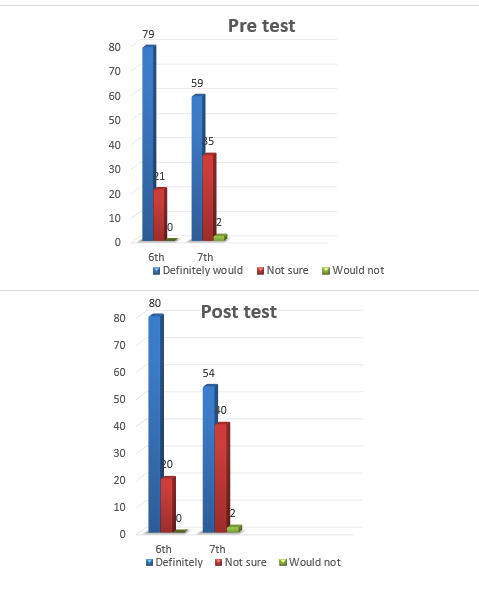
Table 6: 6th and 7th graders pre test and post test responses to question 6.
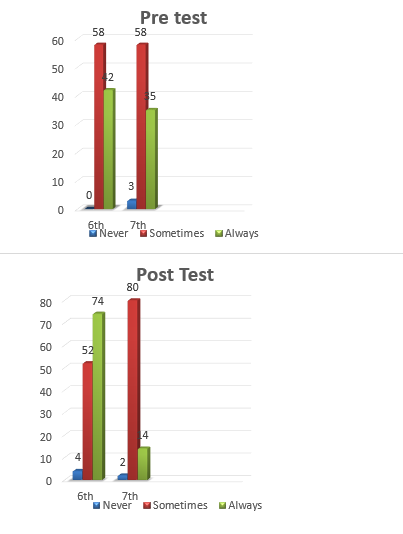
Table 7: 6th and 7th graders pre test and post test responses to question 7.
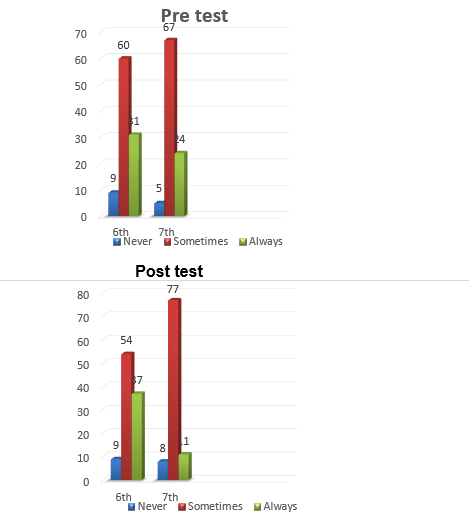
Table 8: 6th and 7th graders pre test and post test responses to question 8.
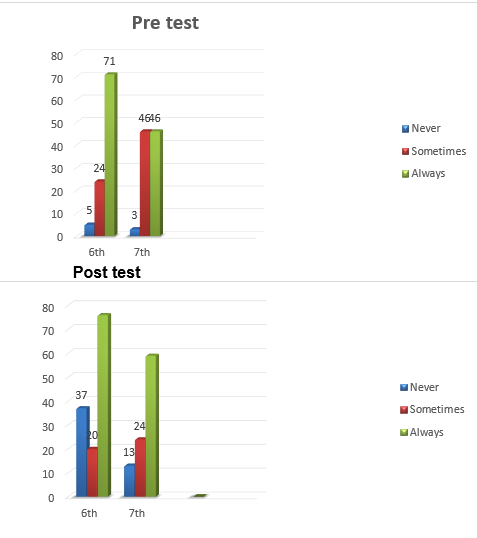
Table 9: 6th and 7th graders pre test and post test responses to question 9
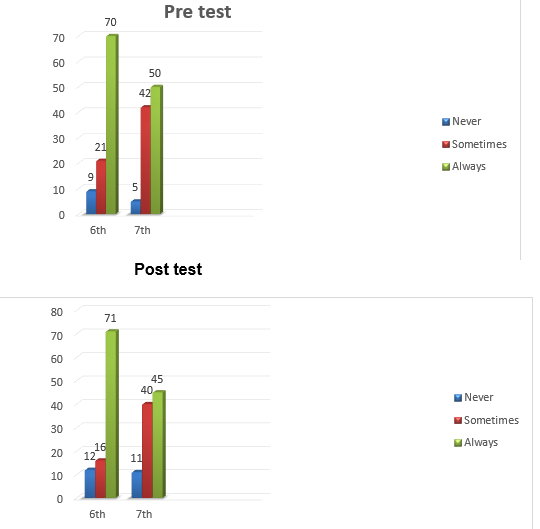
Table 10: 6th and 7th graders pre test and post test responses to question 10.
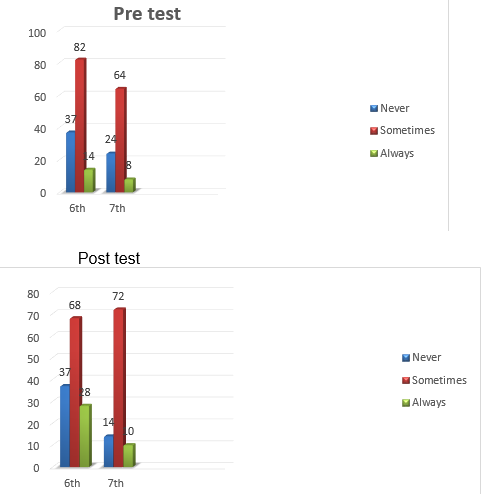
Table 11: 6th and 7th graders pre test and post test responses to question 11.
