Abstract
In this study, the aim was to determine if sickle cell anemia is uniquely common among the Blacks of sub-Sahara descent. Several studies have suggested that indeed this disease is not only common among the African Americans but also people living in sub-Sahara Africa. The review of the existing literature affirms that indeed sub-Sahara has the highest prevalence of sickle cell anemia, with countries like Uganda recording the highest rate of 45% compared to United Kingdom’s less than 1%. The studies reveal that this is a problem that is caused by harsh environmental conditions that made it necessary to develop natural defense against malaria. The gene mutation protected them from malaria, but it left them more susceptible to sickle cell anemia because of the abnormalities of the red blood cells. The study has concluded that the high prevalence of sickle cell anemia has nothing to do with skin color or social status of the Blacks.
Introduction
Sickle cell anemia is a genetic problem that scientists have been trying to find a solution to over the past several years since its discovery over fifty years ago. Brown (2006, p. 41) defines sickle cell anemia as “a severe hereditary form of anemia in which a mutated form of hemoglobin distorts the red blood cells into a crescent shape at low oxygen levels.” Vernon Ingram was able to identify the abnormalities in amino acid sequence (β-globin chain), and his discoveries laid the ground for further research about this genetic disease (Eric 2007). Recent studies have suggested that sickle cell anemia is more prevalent among the Blacks, especially those of sub-Saharan descent. The objective of this study is to determine if sickle-cell anemia is uniquely common among the Blacks of sub-Saharan descent. The study will try to answer the following hypothesis question.
Is sickle-cell anemia uniquely common among the Blacks of Sub-Saharan descent?
The study will try to determine if indeed this genetic problem is uniquely common among the Blacks all over the world, especially those who are currently living in sub-Sahara Africa or those whose ancestry can be traced to this region. This research is very important because it will motivate further study among the affected population to determine if there is something unique about the environment around this region that has direct impacts on the genetic composition of people. It may be a step towards finding a permanent solution to this problem.
Discussion
Sickle-cell anemia is prevalent among the African Americans
Recent studies have strongly suggested that sickle cell is a black disease that affects more Blacks than any other race in the world. A research conducted by Center for Disease Control and Prevention revealed that sickle-cell anemia is more common among the African Americans, especially those whose ancestry can be traced to sub-Sahara Africa (Hill 2005). In this comparative analysis, it was determined that about 100,000 people suffer from sickle cell anemia in the United States (Smith 2008). For every 365 African Americans, one of them suffers from this genetic problem. The race with the second worst record was the Hispanic-Americans. One out of every 16,300 Hispanic Americans suffers from sickle-cell anemia. The problem is rare among the Whites. It is clear from this comparative analysis that the problem is serious among the African Americans.
A study by Tapper (2000) paints even a sadder picture that 1 out of every 13 African Americans are born with traits of sickle cell anemia. These studies strongly suggest that most of the affected population moved to the United States from sub-Sahara Africa either during the era of slave trade or after. About 8% of the African Americans have sickle cell trait (SCT), which means that although they do not suffer from the disease, they carry one defective gene (Bloom 2004). These carriers also have high chances of giving birth to a child with abnormal hemoglobin, especially in cases where both parents have sickle cell trait. The genetic abnormality can be passed on to many generations without anyone getting affected (Dickey et al. 2006). Given that it is often difficult to trace health status of family members in the family tree beyond the fourth or fifth generation, sometimes one may not realize that a close relative had the problem at one time. One may not realize that this has been a problem affecting members of the family for the past several generations. That is why it was not until recently that the scientists were able to determine that this problem is very common among the African Americans with ancestry from sub-Sahara Africa.
According to Higgins (2012), scientists believe that the gene mutation that took several centuries ago in the hemoglobin of the ancestors of these African Americans have been inherited by their great grand children over the years. One of the best ways of fighting this disease from one generation to the other is through marriage between a carrier and a healthy individual. This reduces chances of any of the siblings being a carrier to 0.25 (Russell 2009). It also eliminates chances that the offspring of such a couple will suffer from such a disease significantly. Boyle (2008) says that most of the carriers of this disease do not always realize that they do have distorted hemoglobin as long as they do not develop related complications. It is rare to find a situation where a couple goes for a test of the hemoglobin before having a child. In fact, Kumar (2012) says that majority of the Americans do not have full knowledge of this disease. As such, it has been difficult to fight the disease among the African Americans who have high prevalence of being carriers of the distorted red blood cells.
Sickle cell anemia and socioeconomic status
According to Isichei (1997), there is often a perception among the international community that sub-Saharan region is synonymous to poverty, high level of illiteracy, constant conflicts, famine, and all forms of misfortunes that one can imagine in the modern society. Given that the recent studies have consistently indicated that people living in this region or those whose parents or ancestors moved from this region to other parts of the world have a higher rate of being anemic than people from other parts of the world, there is a feeling that this is a problem that is common among the poor (Elk and Landrine 2012). Others may even want to associate it with limited access to healthcare facilities. However, Brown (2006) says that sickle cell anemia is a problem that affects both the rich and the poor. The statistics have shown that there is a close relationship between the origin of people (whether or not their ancestors came from sub-Sahara Africa) and the prevalence of this disease. However, there was no meaningful link between one’s social status and the prevalence of the disease. The rich and the poor have almost the same risk rate (Higgins 2012).
The only difference that was detected was the ability to manage the disease. Sickle cell anemia, just like any other form of cancer, can easily be managed if it is detected early and interventions are taken as soon as possible to arrest the situation early enough (Goroll and Mulley 2009). When it is allowed to advance, then the treatment does not only become more expensive, but the success rates also go down. The rich are able to detect the problem early because of their regular health-checks, a luxury that the poor cannot afford. For that reason, the rich have a better chance of managing this disease than the poor. However, the rate of occurrence is not in any way related to one’s social status. This argument effectively rules out any perception that this disease is possibly caused by the inability of the African Americans to maintain a given standard of health. It confirms that this problem is common among the African Americans of sub-Saharan descent irrespective of their social status.
The awareness campaign going on about sickle cell anemia is having a positive impact in the fight against this disease among the rich than it is among the poor. As stated above, when the two parents are carriers of the distorted red blood cells but do not suffer from the disease, they have a very high chance (0.5) of having a child who is anemic (Kumar 2012). The poor may not have time and resources to go and test whether they are carriers or healthy parents. In fact, the civic education about anemia is rarely taken seriously by this group. However, the rich are often concerned about their health. They can afford and are willing to do such tests to ensure that they avoid cases where both parents are carriers of the distorted red blood cells (Russell 2009). They significantly reduce chances of having children who are either anemic or carriers of the cell.
Sub-Sahara has the highest prevalence of sickle cell anemia
As discussed in the section above, scholars have suggested that sickle cell anemia is prevalent among the African Americans, especially those who migrate from this region to the United States. These claims can only be valid if studies indicate that sub-Saharan countries have recorded the highest incidences of sickle cell anemia than any other country in the world. A study by Andrews and Boyle (2008) shows that a number of countries in sub-Sahara Africa have recorded the highest incidences of sickle cell anemia, a clear confirmation that this problem is more prevalent among people living in this region. In West Africa, Ghana and Nigeria, which are the leading economies in this region, have a prevalence of over 20%. This is worrying given that a country such as the United Kingdom has a prevalence of less than 1% (Engleberg and Schaechter 2007). The situation gets worse towards central and East Africa.
In Central African Republic and Democratic Republic of Congo have prevalence levels of about 30%. The Republic of Uganda has one of the worst prevalence rates that have ever been recorded in the recent times, standing at 45% (Smith and Passik 2008). This is a major concern given that most of the cases go unnoticed because some of these cases are never taken to hospital. Raskó and Downes (2005) give an example of the people of Karamoja in East Uganda, Pokot and Turkana of Northern, and some people staying in southern part of South Sudan who rarely go to hospital for medical attention. They rely on traditional midwives to help them in delivery. When they fall sick, they go to traditional medicine men who know nothing about sickle cell anemia. The hospitals are either so far that they find it almost impossible to access them due to the poor infrastructure or their religious beliefs prohibit them from going to hospitals for any form of medications or check-ups. As such, the statistics given about the prevalence of sickle-cell anemia in some parts of African countries such as Uganda, Kenya, South Sudan, and Congo are underestimated because those who are at the greatest risk are not covered (Pace 2007). They die prematurely without the cause of their death being categorically stated as sickle cell anemia. This is a further confirmation that indeed there is a high prevalence of this disease in this region.
Sickle cell anemia is not a ‘black’ disease
According to Alcena (2013), there is a wrong perception among the people who have been critically reviewing the prevalence of sickle cell anemia that this is a ‘black’ disease. The researcher agrees with other scholars that indeed the problem is more prevalent in sub-Sahara Africa than it is in any other part of the world. The researcher also agrees with the argument that this disease has been common among the people who migrated from this region to other parts of the world. However, the study seeks to explain that this is a problem that is not in any way related to the color of the skin. Collins (2006) says that sub-Sahara Africa is known for the high prevalence of malaria. This disease is more common in this region than it is in any other parts of the world. Kumar (2012) notes that when missionaries and explorers from Europe first came to Africa, many of them died of malaria, but the locals were able to survive in that hostile environment even though they did not have medicine to treat this disease. People living in sub-Saharan Africa have developed resistance to malaria because of the gene variant.
On the flipside, the variation of gene that has made them resistant to malaria makes them vulnerable to sickle cell because the variation occurs in the red blood cells (RBC). This was a natural evolution caused by the fact that malaria is a more deadly disease than sickle cell anemia. As such, majority of the people who have lived in sub-Sahara Africa for centuries- especially those living in malaria belt regions- have had some form of gene mutation as a way of adapting to the harsh climate. As Steinberg (2001) notes, it was the only way of surviving in this region given that treatment for malaria was not available at that time. The mutation had nothing to do with the skin color but the nature of the environment in this region (Russell 2009). As such, although the disease is common among the African Americans of sub-Sahara descent, it is not a problem of the Blacks.
Sickle cell anemia affects other populations
Sickle cell anemia also affects people from other parts of the world who have never been to Africa and do not trace their ancestry to sub-Sahara Africa. The figure below shows some of the regions around the world where the problem of sickle cell anemia is as bad as in some parts of Africa.
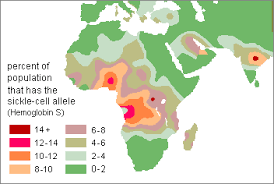
As shown in the above figure, a section of Middle East, the Mediterranean, and parts of India also have high cases of sickle cell anemia. According to Montalembert (2008), the high prevalence of this disease in this region is not caused by high rates of immigration into this region from sub-Sahara Africa as is the case in the United States, South American continent and Europe. In fact, Lehmann (2003) says that the number of people migrating from India to Africa outnumbers those moving from Africa to India. These regions share one common environmental problem, and that is the high prevalence of malaria spread by female anopheles mosquito. The prevalence of malaria in this region has resulted into gene mutation to help the residents form a natural defense against the disease (Lomus 2011). This is a further confirmation that this problem is caused by environmental factors other than the skin color. Wu (2003) says that it is true that sub-Sahara Africa and people who at one time migrated from this region have high prevalence of sickle cell anemia because of the gene mutation that was necessary for their own survival or the survival of their ancestors.
Conclusion
This investigative research has effectively affirmed the claim that sickle cell anemia is uniquely common among the Blacks of sub-Sahara descent. Emphasis should not be laid on their skin color as being black, or on their social status as being relatively poor compared to the Whites. Studies have shown that skin color and social status have nothing to do with the problem of sickle-cell anemia. The disease is prevalent among the people whose ancestry can be traced to sub-Sahara Africa because of the mutation of the gene that was necessary to make them develop natural defense against malaria. The fact that the problem also affects non-Black populations who have never been to Africa such as the Indians, shows that this is a problem that is caused by the environment than it is by skin color.
References
Alcena V. 2013. African Americans and medical diseases: An American health care crisis that is crying for help and actions. Pittsburgh, Pennsylvania: RoseDog Books.
Andrews MM, Boyle JS. 2008. Transcultural concepts in nursing care. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Bloom M. 2004. Understanding Sickle Cell Disease. Jackson: University Press of Mississippi.
Brown RT. 2006. Comprehensive Handbook of Childhood Cancer and Sickle Cell Disease: A Biopsychosocial Approach. New York: Oxford University Press.
Collins CF. 2006. African American women’s health and social issues. Westport, Conn: Praeger Publishers.
Dickey S, Greenberg C, and Bowden VR. 2006. Children and their families: The continuum of care. Philadelphia, PA: Lippincott Williams & Wilkins.
Elk R, Landrine H. 2012. Cancer disparities: Causes and evidence-based solutions. New York: Springer Pub. Co.
Engleberg NC, Schaechter M. 2007. Schaechter’s mechanisms of microbial disease. Philadelphia: Lippincott Williams & Wilkins.
Eric MH. Addressing Nature-Of-Science Core Tenets with the History of Science: An Example with Sickle-Cell Anemia & Malaria. The American Biology Teacher. 2007; 69: 467–472.
Foy H, Kondi A, Jelliffe DB, Humphreys J. Sickle-Cell Trait in Africans. The British Medical Journal. 2002; 2: 41–43.
Goroll A, Mulley, AG. 2009. Primary care medicine: Office evaluation and management of the adult patient. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins.
Higgins C. 2012. Understanding Laboratory Investigations: A Guide for Nurses, Midwives and Health Professionals. Chicester: Wiley.
Hill S. 2005. Managing sickle cell disease in low-income families. Philadelphia: Temple University Press.
Isichei E. 1997. A history of African societies to 1870. Cambridge: Cambridge Univ. Press.
Kumar D. 2012. Genomics and health in the developing world. Oxford: Oxford University Press.
Lehmann H. Sickle-Cell Anaemia. The British Medical Journal. 2003; 2: 1217–1218.
Lomus K. 2011. The Work of Patient Advocacy. New York: Princeton University Press.
Montalembert M. Management of Sickle Cell Disease.BMJ: British Medical Journal. 2008; 337: 626–630.
Pace B. 2007. Renaissance of sickle cell disease research in the genome era. London: Imperial College Press.
Raskó I, Downes CS. 2005. Genes in medicine: Molecular biology and human genetic disorders. London: Chapman & Hall.
Russell A. 2009. Lecture notes. Chichester, UK: Wiley-Blackwell.
Smith HS, Passik SD. 2008. Pain and chemical dependency. Oxford: Oxford University Press.
Smith J. 2008. Health inequalities: Written evidence. London: TSO.
Steinberg MH. 2001. Disorders of hemoglobin: Genetics, pathophysiology, and clinical management. Cambridge: Cambridge Univ. Press.
Tapper M. 2000. In the blood: Sickle cell anemia and the politics of race. Philadelphia: Univ. of Pennsylvania Press.
Wu J. Review of Contagious Divides: Epidemics and Race in San Francisco’s Chinatown. Social History. 2003; 28: 136–138.